Unicompartmental knee arthroplasty has emerged as an effective method for treating end-stage medial compartment osteoarthritis because it preserves the surrounding anatomical structures of the knee joint and maintains the physiological characteristics of lower extremity motion [17, 18]. This procedure is characterized by rapid postoperative recovery and positive patient experiences. When performing unicompartmental knee arthroplasty (UKA), the primary consideration should be precision. Unlike total knee arthroplasty (TKA), UKA has a lower tolerance for error [19]. Improper implant positioning, malalignment, and ligament imbalance can all lead to UKA failure. Numerous studies have demonstrated that, compared with conventional techniques, robotic-assisted surgery significantly improves the accuracy of bone preparation, implant positioning, implant alignment, and soft-tissue balancing [20, 21]. Khow et al. [22]. conducted a follow-up study of 264 cases of medial unicompartmental arthroplasty with fixed-bearing prostheses to determine the effect of femoral component positioning on the longevity of these implants. They measured the coronal angles of the femoral and tibial components on postoperative radiographs and categorized those with varus or valgus angles greater than 3° as the OG group and those with angles less than 3° as the AG group. Follow-up examinations were performed at six months, two years, and ten years postoperatively. They found that both prosthesis lifetime and Oxford Knee Score (OKS) scores were lower in the OG group than in the AG group, concluding that in fixed-bearing medial unicompartmental arthroplasty, a femoral component varus/valgus angle greater than 3° significantly affects long-term efficacy. Diezi et al. [23] previously suggested that varus/valgus angles of the tibial component exceeding 5° would exacerbate wear on the tibial side of fixed bearings. Innocenti et al. performed a finite element analysis of the stress distribution of the UKA tibial component and polyethylene liner under 6° varus/valgus conditions. The results indicated that the lowest stress occurred when the tibial component was in a neutral position or 3° of valgus.
It is well known that precise bone resection and accurate implant positioning are critical to the clinical outcomes and long-term survival of unicompartmental knee arthroplasty (UKA). Intraoperative malpositioning of the prosthesis may lead to under- or over-correction of lower limb alignment, potentially resulting in early prosthetic loosening and the development of osteoarthritis in the contralateral compartment [24,25,26,27]. Previous studies have demonstrated that using a threshold of 3° deviation for implant alignment, the success rate of prosthetic placement in robotic-assisted UKA was 87%, compared to only 28% in the conventional surgery group [28]. The results of this study revealed that at the final follow-up, the range of coronal femoral component alignment deviation measured radiographically was − 2.60° to 2.30°, with a mean of (0.84 ± 1.77)°, while the tibial component alignment deviation ranged from − 0.90° to 1.50°, with a mean of (0.56 ± 0.83)°, all within the 3° threshold. Therefore, we have reason to believe that the NATON robotic system can effectively assist clinicians in achieving optimal positioning of the implanted prosthesis.
Posterior tibial slope (PTS) is also critical to the performance of the tibial component. The average PTS in normal adults is 8°. Excessive posterior tilt of the tibial prosthesis can increase stress on the posterior tibial bone, leading to ACL tears and prosthesis loosening [29]. Hernigou retrospectively analyzed 18 patients with anterior cruciate ligament deficiency who underwent unicompartmental arthroplasty with a follow-up of up to 16 years. In this study, none of the 11 patients with PTS less than 5° showed prosthetic loosening and all prostheses remained in place without revision. In contrast, the seven patients with a PTS greater than 8° required revision surgery. The authors also recommended that the PTS be less than 7° [30]. In this study, postoperative femoral component angles were maintained within 3°, tibial varus/valgus angles were maintained within 1°, and posterior tibial slope was maintained below 7°, meeting the standards established by the aforementioned studies. This approach prolongs the life of the prosthesis and demonstrated the precision of the robotic implantation procedure.
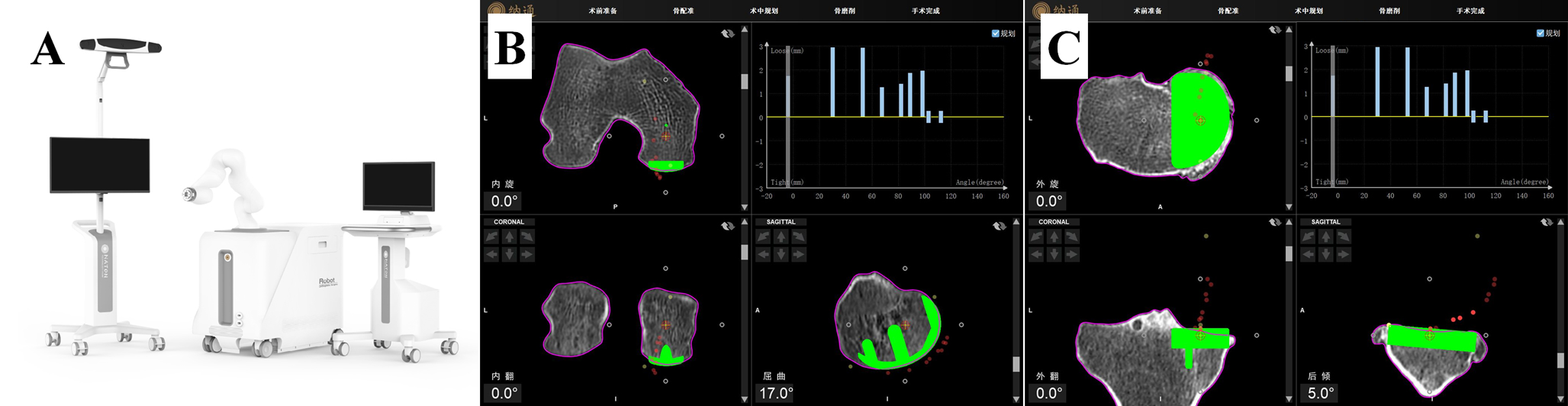
Batailler et al. conducted a randomized controlled clinical trial comparing 80 patients who underwent robotic-assisted unicompartmental knee arthroplasty with 80 patients who underwent traditional unicompartmental knee arthroplasty from 2013 to 2017, with an average follow-up of 19.7 months. The results showed that the robotic unicompartmental knee arthroplasty group had better clinical outcomes and a lower rate of prosthesis loosening [31]. Similarly, Foissey et al. compared 197 cases of robotic-assisted monondylar replacement with 156 cases of patients in the traditional surgery group, with a mean follow-up of 61.3 ± 24.0 months, and evaluated related indicators such as lower extremity HKA angle, medial tibial tilt angle, posterior tibial flat prosthesis tilt angle, and joint line height, indicating that robotic-assisted monondylar replacement has its advantages. At the last follow-up, implant survival rates were higher in the robotic group [32]. In the past, the appropriate prosthesis type and good prosthesis position relied on preoperative 2D imaging and the surgeon’s surgical experience, which can lead to large errors in prosthesis size and position and inconsistencies in postoperative outcomes between different surgeons. The NATO Robotic-Assisted System is based on the pre-operative 3D reconstruction of the hip, knee, and ankle using thin-slice CT scans (< 1 mm) to define the relevant lines of force, osteotomy thickness, and prosthesis position, which is undoubtedly more intuitive and accurate. In the actual surgical procedure, we will adjust the osteotomy volume and prosthesis position according to the preoperative knee flexion/extension gap before the osteotomy as well as the prosthesis trajectory, and we usually reserve 2–3 mm of flexion/extension gap, which is sometimes difficult to be precise in traditional surgery, but easier to do in robotic surgery, reflecting the precision and consistency of the osteotomy and prosthesis position, which is key to the survival of the prosthesis.
Dunbar et al. [33]performed unicompartmental knee arthroplasty using the MAKO robotic system on 20 knees. The study required preoperative planning and postoperative imaging to demonstrate prosthesis placement error of less than 1.6 mm and varus/valgus alignment within 3°. Post-operative x-ray and CT results showed that the femoral prosthetic error averaged 0.8 mm and 0.9°, while the tibial prosthetic error averaged 0.9 mm and 1.7°, demonstrating the precision of the MAKO robotic system. Previous studies have mainly focused on imported robotic systems, while this study shows that the domestic Naton robot achieves satisfactory early results in terms of both prosthesis placement accuracy and patient functional improvement.
Kim et al. suggested that poor lower extremity power lines are also a common cause of revision, and we need to focus on correcting lower extremity power lines in robotic-assisted surgery at the same time [34]. We aim to restore the mechanical axis of the lower limb to neutral or near-neutral alignment. Thanks to the robotic system’s precise assessment of soft tissue tension, the surgeon can finely adjust the preoperative plan during surgery to accurately control the medial compartment gap, maintaining it within the ideal range of 2–3 mm throughout the full range of flexion and extension. This ensures that the contact trajectory between the femoral and tibial components remains in an optimal state. Additionally, with the real-time navigation provided by the robotic system, the surgeon can continuously monitor the lower limb alignment, avoiding excessive medial tightness and knee valgus. Traditional surgery relies heavily on preoperative full-length lower limb radiographs and the surgeon’s experience, whereas in robotic-assisted surgery, we simply follow the preoperatively planned alignment for osteotomy and implant positioning. This simplifies the reliance on subjective experience, enabling the restoration of normal knee kinematics and soft tissue balance, thereby improving postoperative range of motion and patient satisfaction.
Excessive intraoperative traction of the knee joint and repeated osteotomies may lead to soft tissue damage and hypertrophic scar formation within the knee, resulting in stiffness and pain during knee movement [35]. The precise navigation provided by the NATON robotic system eliminates the need for multiple osteotomies, thereby reducing trauma to the soft tissues surrounding the knee. This not only helps alleviate postoperative pain caused by soft tissue contracture but also minimizes scar tissue formation, enhancing the patient’s early postoperative mobility. Notably, in terms of safety, the precise navigation of the NATON robotic system prevents excessive bone resection. The protective mechanism of automatic power disconnection in the robotic arm ensures that critical vessels and nerves around the knee are not injured during surgery, significantly reducing surgical risks.
In a survival analysis of robotic versus non-robotic unicondylar replacement with up to three years of follow-up, St Mart et al. mentioned that unicondylar replacement with the Mako robot had a higher rate of early revision, mostly due to early infectious factors rather than prosthesis position [36]. In our study, no complications were found in any of the robotic surgery patients, although this was our first series of Nathon robotic surgery patients, so there is reason to believe that robotic surgery is safe.
The use of the Naton robot for unicompartmental knee arthroplasty involves a learning curve. In the early stages, the need for intraoperative registration and frequent calibration complicates the surgical process, resulting in an average operative time of approximately 100 min. However, as the surgical team becomes more familiar with robotic surgery, the average operative time can be reduced to approximately 50 min, a significant improvement. To optimize robotic surgery, it is advisable to develop a dedicated team that is thoroughly trained in the robotic surgical procedures and steps. This coordinated effort can further reduce surgical time [37]. In addition, regular maintenance and upkeep of the robotic hardware and software are essential, resulting in higher surgical costs compared to traditional methods. In addition, there are limitations in the compatibility of unicompartmental prosthesis designs from different manufacturers. Currently, the Naton robot is only registered for the Link fixed-bearing prosthesis and the Zhengtian fixed-bearing unicompartmental prosthesis, which limits the variety of prosthesis options available to patients.



Comments (0)