
Remember me
During the study period, 112 patients with proven or probable/putative IA were identified.
Characteristics of patients with IAThe detailed characteristics of patients with IA are available in Table 1.
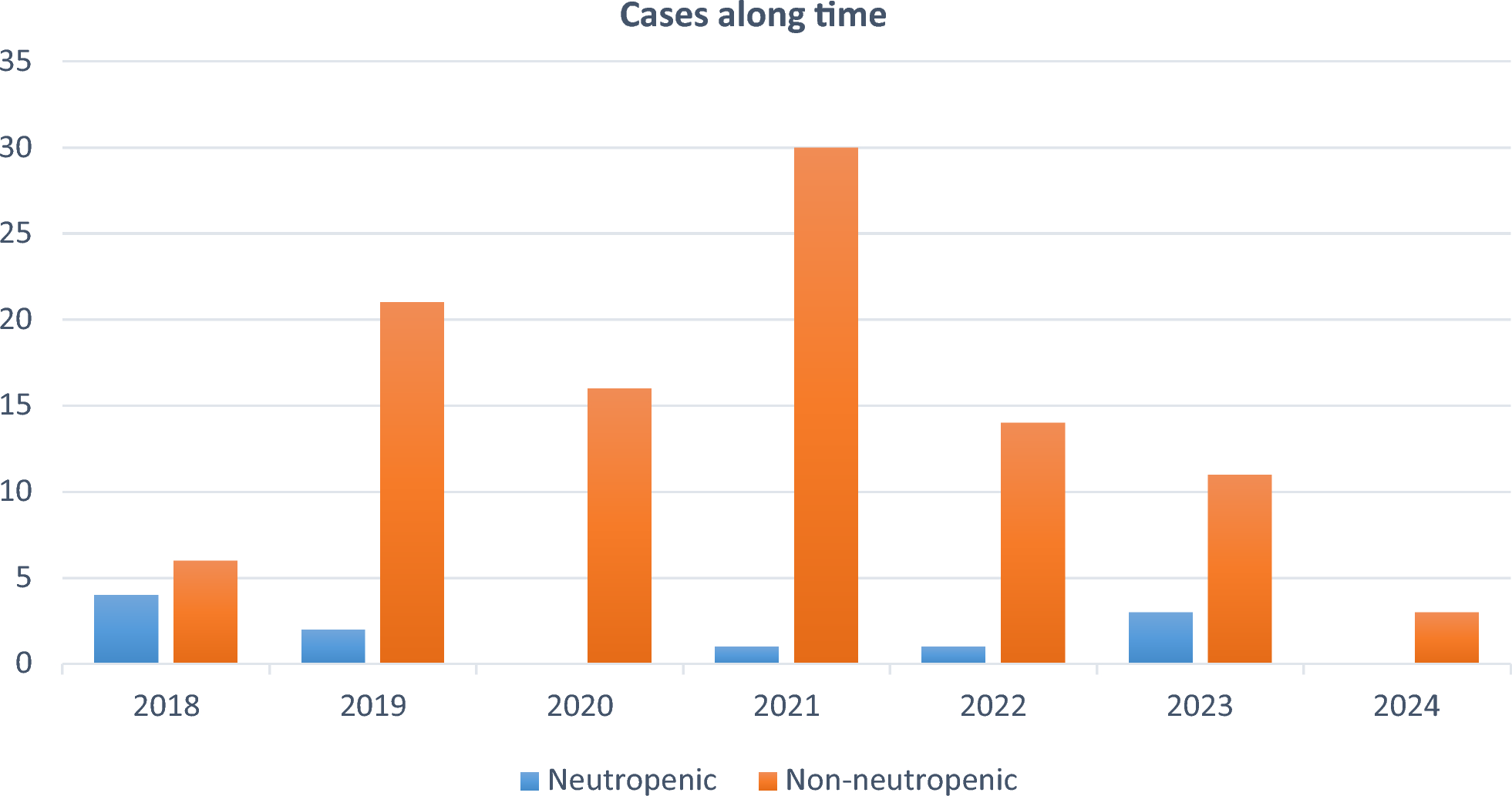
Only 11 patients (9.8%) were neutropenic at the time of IA diagnosis or in the previous month. Prevalence of IA among neutropenic and non-neutropenic patients evolved along time (Fig. 1), with a sharp increase in non-neutropenic cases during COVID first waves, and a general predominance of non-neutropenic hosts in the whole series, with a trend to a decrease in neutropenic cases.
Fig. 1
Evolution of cases of invasive aspergillosis along the study period
Main underlying conditions were previous corticosteroid use (71.4%), chronic lung disease (42.9%), lung transplantation (31.3%), SARS-CoV2 infection (26.8%), CMV infection (25.9%), chronic kidney disease 21.4%, hematological diseases (19.6%) and oncological disease 9 (8%). All patients with CMV reactivation had, in addition, another underlying disease (17 COVID, 3 HSCT, 10 SOT, 5 hematological malignancies, 1 HIV AIDS stage with IA at diagnosis and one with severe exacerbated pneumoconiosis with admission to the intensive care unit).
The majority of IA cases 88 (78.6%) were considered probable/putative. The most commonly involved organ was the lung in 100 (89.3%) patients. Six cases (5.4%) presented disseminated infection.
28 patients (25%) had a 18F-FDG-PET-TC performed in addition to conventional imaging (53.6% staging, 14.3% monitoring and 32.1% due to persistent fever).
Serum galactomannan (GM) was performed in 81 patients, with a 28.4% positivity rate. 78 patients (71.4%) underwent bronchoscopy. Among 41 GM tests performed in BAL, 32 (78%) were positive.
In 90 (80.4%) cases a positive Aspergillus culture was available. The most frequent species was A. fumigatus sensu stricto (53 [56.9%]). Other species were: A. terreus (7 [7.5%]), A. flavus (6 [6.5%]), and A. niger (4 [4.3%]). As many as 13/93 (14%) isolates were identified as cryptic species, including among Fumigati: Neosartorya udagawae (1), A. lentulus (8), A. fumigatiaffinis (1); among Terrei: A. hortai (2); among Nidulans: A. spinulosporus (1). Evolution over the years of cryptic species IA is shown in Fig. 2.
Fig. 2
Evolution over the years of cryptic species
The distribution of resistance is summarized in Tables 2, 3. Resistance to Voriconazole and Isavuconazole was found only in 2 (3.8%) A. fumigatus sensu stricto isolates, and 1 (1.9%) isolate was resistant to Posaconazole, Itraconazole and Amphotericin B. One of these presented the TR34-L98H mutation.
Table 2 Resistance in Fumigati sectionTable 3 MIC of the rest of the isolated Aspergillus speciesAmong the cryptic species of the Fumigati family, resistance was higher with 10 isolates with Voriconazole MIC ≥ 2, 8 with Isavuconazole MIC > 2 and 7 Amphotericin B MIC ≥ 2.
Breakthrough IFI was detected in 41/112 (36.6%) cases and in more than half of them (21/41 cases, 51.2%), the isolate was resistant to the prior antifungal.
The most frequently used empirical therapies were Isavuconazole (60 [53.6%]) and Voriconazole (37 [33%]). Resistance to empirical therapy was observed in 11/112 (9.8%) patients. The most common targeted antifungals were Isavuconazole (63 [56.3%]), Voriconazole (25 [22.3%]) and L-Amphotericin B (25 [22.3%]).
Among breakthrough IA, the most common empirical antifungal therapy was Voriconazole in 4 patients (8.9%), Isavuconazole in 35 patients (77.8%) and L- Amphotericin B in 6 patients (13.3%). Out of them, 7 (15.6%) cases were resistant to the empirical antifungal.
Among SOT, 5 recipients (4.5%) lost the graft as a consequence of IA. IA motivated a delay of chemotherapy or HSCT in 8 patients (7.1%). In-hospital mortality rate was 33.9% (38/112).
Differences between neutropenic and non-neutropenic patientsDifferences between neutropenic and non-neutropenic patients were found regarding underlying diseases, clinical and radiological presentation, microbiological data and antifungal therapy (Fig. 3).
Fig. 3
Differences between neutropenic and non-neutropenic patients
Underlying diseasesThe most common underlying disease in non-neutropenic was SOT, especially lung transplant in 35/48 (34.7%; p-value 0.016), whereas in neutropenic, it was hematological disease in all patients (100%; p-value 0.0001), and receipt of chemotherapy in 9 cases (81.8%; p-value 0.0001).
Previous corticoid use was detected more frequently in non-neutropenic, 78 (77.2%), as compared to 2 (18.2%) among neutropenic (p-value 0.0001).
Regarding infections that are known to constitute a risk factor for aspergillosis, in non-neutropenic, 30 cases of SARS-CoV2 infection (29.7%; p-value 0.035), 4 of influenza (3.9%) and 29 CMV reactivations (28.7%; p-value 0.037%) were diagnosed in the previous month, in contrast with 0 cases in neutropenic patients. We detected 9 cases of IA associated with solid tumors, 6 (66.7%) of them were lung cancer and the other 3 were metastatic cancer. The most common presentation was pulmonary aspergillosis (77.8%), with cavitated nodules being the most common finding. 2 of the patients had previous cavities related to the oncological pathology.
Clinical presentation and microbiological dataThe most widespread form of presentation was pulmonary aspergillosis in both groups, in 88.1% of non-neutropenic and in 100% of neutropenic, but non-neutropenic presented other sites of involvement as well.
Six cases of disseminated infection were diagnosed in non-neutropenic patients (5.9%). The characteristics of disseminated aspergillosis are shown in Table 4. Disseminated cases presented mainly in SOT recipients, although one case occurred in a patient with COVID-19 and significant immunosuppression and another had a probable endovascular source. Two of them survived, in keeping with a reduction of immunosuppression, that in the case of the kidney transplant conveyed the loss of the graft.
Table 4 Characteristics of disseminated invasive aspergillosisAmong the included patients with IA, ground glass opacities (81.8% [9/11] vs 46.8% [44/94]; p-value 0.052) and lung nodules (72.7% [8/11] vs 43.6% [41/94]; p-value 0.108) with halo sign (45.5% [5/11] vs 7.4% [7/94]; p-value 0.003[NS]) were more common in patients with neutropenia than in those without neutropenia. In non-neutropenic, there was a wider variety of chest CT findings.
Positive cultures were detected more often in non-neutropenic (85 [84.2%]), as compared to neutropenic (6 [54.5%]); more information about positive cultures is shown in Table 5. In both groups, the most frequently isolated species was A. fumigatus, and there were no significant differences in the distribution of Aspergillus species, although cryptic species were more common in neutropenic (28.6% versus 12.8%, p-value 0.252), and some species were found only in non-neutropenic (A. flavus, A. terreus, A. nidulans…).
Table 5 Number of samples with positive culture in the complete cohortSerum GM was positive more frequently in the neutropenic group, 5 (45.5%) versus 18 (25.7%) non-neutropenic (p-value 0.137). Among the 4 IAPA cases, only 3 had GM tested in serum, with 33.3% positivity compared to 40% GM positivity in 30 CAPA cases. All neutropenic patients underwent bronchoscopy (100%) detecting a positive GM in BAL in 6 cases (66.7%) compared to 26 (81.3%) positive GM in BAL in non-neutropenic (p-value 0.304).
Neutropenic patients were receiving previous antifungals more often, and consequently presented breakthrough IFI in a greater proportion: 7 (63.6%) neutropenic compared to 34 (33.7%) non-neutropenic. The most commonly used prophylaxes in neutropenic were Fluconazole or Posaconazole, 3 each (42.9%), while in non-neutropenic it was nebulized L-Amphotericin B in 33 (97.1%). In 4 (57.1%) neutropenic and 17 (50%) non-neutropenic patients the Aspergillus species that caused the breakthrough infection was resistant to the antifungal used for prophylaxis.
In neutropenic cases, the most common used antifungal was intravenous L-Amphotericin B, both empirically (54.5% [6/11] vs 5.9% [6/101]) and as targeted treatment (63.6% [7/11] vs 17.8% [18/101]). On the contrary, in non-neutropenic patients, Isavuconazole was the most widespread option both empirically (57.4% [58/101] vs 18.2% [2/11]) and as targeted therapy (59.4% [60/101] vs 27.3% [3/11]), respectively.
There were no significant differences in mortality, although it was higher among neutropenic patients (45.5% [5/11] versus 32.7% [33/101]) in non-neutropenic (p-value 0.685).
Characteristics of patients with hematological diseaseThe characteristics of patients with IA and hematological disease are summarized in Table 6.
Table 6 Invasive aspergillosis in hematological patientsAlmost half of the 22 patients with underlying hematological disease had neutropenia, 10 patients (45.5%), whereas among the 7 (31.8%) patients that had undergone a HSCT, only 2 (20%) were neutropenic. Among patients with IA and hematologic malignancies, chemotherapy was more common in patients with neutropenia than in those without neutropenia (90% [9/10] vs 25% [3/12], p-value 0.004[NS]) while the previous use of steroids (75% [9/12] vs 10% [1/10]; p-value 0.004[NS]) was more frequent in non-neutropenic. 8/22 patients (36.4%) were under new targeted therapies (Ibrutinib, Venetoclax, Dasatinib, bispecific antibodies).
IA presented as persistent fever in 100% neutropenic individuals versus only in 6 (50%) non-neutropenic (p-value 0.009[NS]), while respiratory failure was the most common presentation among non-neutropenic (10 [83.3%]) as compared to neutropenic (5 [50%]) (p-value 0.172).
Pulmonary nodules were the most common imaging finding in both groups (9 [75%] non-neutropenic and 8 [80%] neutropenic), but the halo sign was more prevalent among neutropenic (5) as compared to non-neutropenic (1) (50% vs 8.3%, p-value 0.056).
Breakthrough IFI was seen mainly in neutropenic (6 [60%]) as compared to non-neutropenic (2 [16.7%]) (p-value 0.074).
Comments (0)