Skull base osteomyelitis of the petrous bone
Skull base osteomyelitis of the temporal bone (SBO) is a serious disease due to its topographical localization and the associated high morbidity as well as the often protracted and sometimes frustrating diagnosis and treatment. Depending on the author, high mortality rates between 46% [24] and 70% [30] are described, although to the low prevalence and inconsistent terminology, etiologically different diagnoses are sometimes grouped together.
This results in a mix of different terms such as skull base osteomyelitis, petrous bone osteomyelitis, otitis externa maligna or necrotizing osteomyelitis, which are largely used synonymously depending on the author.
In the context of this case report, the terminology of SBO is used; on the one hand, to emphasize the anatomical brisance in the context of the described course of the disease, on the other hand because classical pathogenesis is often pathogen- and course-related and therefore does not seem to be applicable here.
Common to other case series is above all the clinical symptomatology with otalgia, otorrhea and increasing hearing loss as well as the protracted diagnosis, in this case of more than 8 years. Classically, the diagnosis is made in combination of clinical and radiological findings; histologically, neoplasms (e.g. lymphomas, myelomas, metastases) or immunological-rheumatological differential diagnoses (fibrous dysplasia, an inflammatory pseudotumor, an IgG-4-associated disease, Paget's disease, and various granulomatoses) should be excluded. Successful treatment requires mandatory pathogen detection [22], as a calculated, pathogen-adapted prolonged antibiotic treatment (of at least 12–48 weeks) must be carried out in addition to surgical debridement.
In recent years, the concept of antibiotic stewardship has been developed for the rational planning, implementation and re-evaluation of microbiological diagnostics and antibiotic therapy, which was also essential in diagnosing this case’s atypical infection [13]. Thanks to close interdisciplinary collaboration, it was possible to systematically narrow down the possible bacterial spectrum at the preanalytical stage by including histological findings and the previous unsuccessful antibiotic treatment attempts.
Due to previous surgery and the resulting structural defects, it became increasingly difficult to obtain new pathological and microbiological samples: In purely practical terms, it was often not possible to distinguish intraoperatively between bone osteolysis and previously introduced fatty tissue for obliteration.
We tried to minimize the risk of false-negative pathogen detection by collecting samples as standardized and evidence-based as possible [22, 23]. These minimum microbiological standards include a pre-analytical interdisciplinary consulting, a pausing of the antibiotic therapy preoperatively (in this case of 2 weeks at best [14]), the minimum number of samples required, a minimum sample size of 0.5 mm – 2 mm tissue, the avoidance of swab samples and an evaluation of the most promising transport media and conditions.
Typical pathogen spectrum of petrous osteomyelitis
In current literature, Pseudomonas aeruginosa, Staphylococcus (Staph.) aureus, Staph. epidermidis, Escherichia coli, Salmonella species (spp.), Proteus mirabilis, mycobacteria other than tuberculosis (MOTT), Streptococcus pneumoniae, Treponema pallidum and Klebsiella spp. are described as the most common bacteria causing skull base osteomyelitis. In the context of secondary immunodeficiency (SID) in particular, opportunistic pathogens such as Mycobacterium tuberculosis, Brucella, Nocardia or invasive mycoses have to be considered as well [2, 4, 18, 24]. In more than 30% of cases, the pathogen cannot be detected [4].
Hypogammaglobulinemia after B-CLL
Secondary hypogammaglobulinemia (SHG) as a consequence of B-CLL has been described by various authors: According to them, the occurrence correlates with the length of disease duration, the age of the patients and various comorbidities [9, 21]. Up to 50% of deaths are caused by infections [9, 16, 20], with a particularly high percentage due to secondary immunodeficiencies. In this case, it is not clear whether the SHG is due to the B-CLL itself or to treatment with a B-cell-targeted immunotherapy (BCTT, in this case rituximab) [6, 7, 17] or the cytotoxic alkylants [28] (in this case bendamustine).
M. pneumoniae’s profile
Mycoplasmas as genera of the Mollicutes are some of the smallest known prokaryotes with a size of 0.1 to 0.2 µm and a genome of only 816 kb. Due to the evolutionary loss of basic cellular mechanisms, such as cell wall synthesis, their adaptation to the human host is unique and in parts comparable to that of viruses: This explains the failure of various diagnostic (e.g. Gram or Ziehl–Neelsen stains) or therapeutic approaches (e.g. β-lactam antibiotics, glycopeptides, fosfomycin) targeting bacterial cell wall synthesis. M. pneumoniae is a major cause of community-acquired pneumonia (CAP) and various other extrapulmonary diseases (M. pneumoniae extrapulmonary diseases, MpEPDs). Similar to this case report, many systemic infections or MpEPDs in immunocompromised patients (e.g. with SID) are preceded by a previous respiratory infection [31].
Difficulties in detecting infections with M. pneumoniae
Mycoplasmas cannot be visualized by light microscopy due to the lack of a cell wall, their small size (keyword: Gram stain) and their partially intracellular infestation [31]. Although microbiological culture is still the microbiological method of choice it cannot be recommended for the daily routine diagnosis of infections with M. pneumoniae:
As mycoplasma ‘s growth is inhibited by sodium polyanetholesulfonate, a major component of most commercial culture media, and specific culture media have not made it to routine diagnostics due to effort, other direct testing techniques have been established [31]. Serological tests, such as the monitoring of specific IgM, IgG or IgA titers, show low sensitivity and specificity [10]: Dumke et al. describes various immune evasion mechanisms that cause either a reduced antibody response or survival despite high antibody titers [10]. On the other hand, serological tests cannot be interpreted in the present case due to the secondary immunodeficiency and the immunoglobulin substitution. Although normal IgG and IgM titers were regularly found in the patient's immunological control serology, an almost complete absence of IgA could explain recurrent infections. Both, the particular immune evasion mechanisms and the present SID must be discussed as possible pathomechanisms in the absence of evidence [3].
This explains why nucleic acid detection [25] should be mandatory in patients with substituted hypogammaglobulinemia [15], in this case, detection was performed by 16S rDNA analysis against the P1-gene [8]. The false-negative findings of previous Pan-PCR examinations can be explained either by less sensitivity compared to the species-specific M. pneumoniae-PCR due to the longer length of the PCR-product, or by the complex surgical extraction of samples in the site previously obliterated with abdominal fat. The sensitivity of the P1-gene-based M. pneumoniae TaqMan PCR was calculated in a multi-center study by Dumke et al. [12] (in which the authors of this report took part) as one to five genomes per reaction.
Hyperbaric oxygen therapy as an individualized treatment approach
Hyperbaric oxygen therapy (HBOT) is repeatedly discussed in case series and retrospective studies as an effective adjuvant to the antibiotic treatment of osteomyelitis [5, 18, 19, 26]. On the one hand, the increased oxygen partial pressure has positive effects by inducing neoangiogenesis and thus synergistically improving the tissue’s accessibility of antibiotic therapy, while on the other hand direct bactericidal effects are achieved, e.g. by increasing leukocyte activity [26]. In addition, both, an increase in oxygen-dependent osteoclastic resorption of necrotic bone and a stimulation of fibroblasts for collagen synthesis have been described [26].
Interestingly, M. pneumoniae does not secrete its own toxins, so that local destruction can be attributed to the host's own inflammatory reaction and to reactive oxygen radicals whose bacteriostatic effect is normally targeted by HBOT [29]. Knowing these therapeutic mechanisms, the limited efficacy in this case of infection with M. pneumoniae can be explained by its intracellular survival.
Calculated antibiotic therapy
In treatment of Mycoplasma infections macrolide and tertracycline antibiotics are drugs of first choice, betalactame antibiotics fail due to the missing cell wall synthesis. Testing the bacteria’s resistance was not possible because of the missing cultural evidence. In Germany macrolide resistances are still rare (approx. 3% in pulmonary infections [11]), nevertheless taking the prolonged medical history, the vulnerable anatomy and the already taken place cranial nerve palsies into account, the decision was made to start a combine azithromycin (1 × 500 mg daily) and doxycycline (2 × 100 mg daily) consulting the ABS.
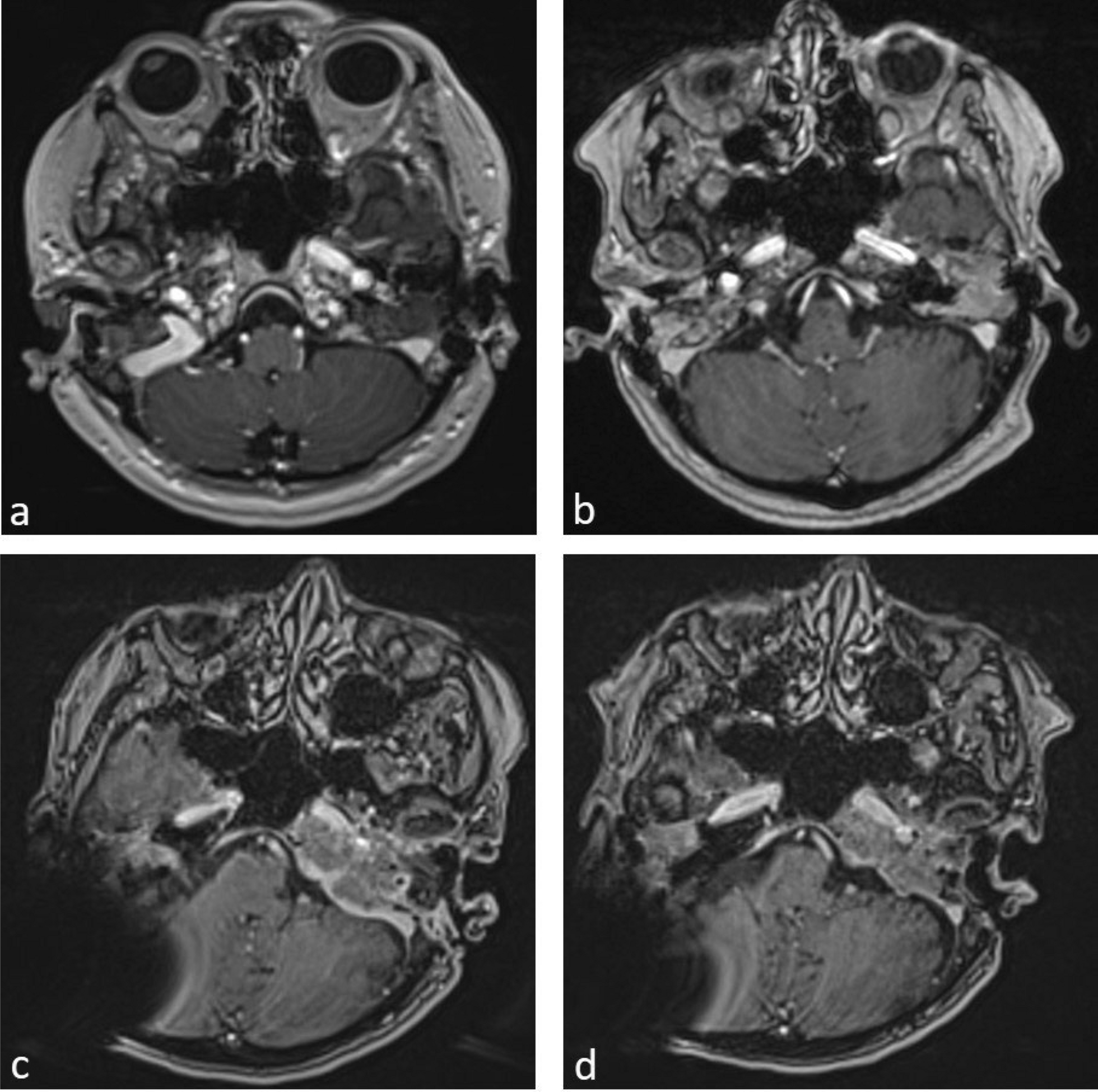
After 6 months of combination therapy, the patient was initially switched to doxycycline monotherapy due to increasing gastrointestinal ADRs. As part of the close clinical follow-up, the cranial nerve palsies continued to decline. Radiologically, the follow-up MRIs showed increasing sclerosis with decreasing CM uptake as a sign of osteomyelitis regression [1] (as shown in Fig. 1).

Comments (0)