Tuberculosis (TB) is a major global health issue caused primarily by Mycobacterium tuberculosis. Despite effective treatment, TB remains a significant health threat. In 2023, there were approximately 10.8 million new TB cases worldwide and 1.25 million deaths, with a notable burden in high TB incidence countries. The WHO’s End TB Strategy aims to reduce TB incidence and mortality through various measures, including rapid detection of drug-resistant strains. Multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB) are particularly challenging, as they require more complex treatment regimens and pose greater public health risks [1].].
World Health Organization (WHO) and United Nation (UN) Member States committed to ending the TB epidemic through the adoption of WHO’s End TB Strategy. The target of this strategy included the annual decline in the TB incidence rate of 4–5% per year by 2020, accelerating to 10% per year by 2025 and then to an average of 17% per year from 2025 to 2035 [2, 3]. Clearly, the emergence and spread of drug resistant tuberculosis represents a serious challenge for the achievement of this goal in many countries [4, 5] Multidrug resistant tuberculosis (MDR-TB), is defined as resistance to isoniazid and rifampicin, the backbone of standard therapy while XDR-TB is defined as a TB caused by Mycobacterium tuberculosis strains that fulfil the definition of MDR/RR-TB and that are also resistant to any fluoroquinolone and at least one additional Group A drug (levofloxacin or moxifloxacin, bedaquiline and linezolid) [6, 7] In high TB burden countries, WHO recommends the rapid detection of Rifampicin resistance (RR) strains, which is used as a proxy for MDR-TB [1].
Globally, an estimated 400 000 people developed multidrug-resistant or rifampicin-resistant TB (MDR/RR-TB) in 2022, with 60,000 MDR/RR-TB cases being reported in Africa [1], where the highest proportion of TB/HIV co-infection is also reported [1, 8]. The most difficult and complicated form of drug resistant TB is known as extensively drug resistant tuberculosis (XDR-TB) reported from several countries, including the Republic of Congo [9].
The Republic of Congo is one of thirty TB high burden countries. In 2023, around 14,370 TB cases were notified in the country, which has an estimated population of 6.14 million (Ref). The overall TB incidence rate was 369 cases per 100,000 inhabitants in the general population and 112 cases per 100,000 inhabitants among individuals with HIV [10] The TB related mortality rate was estimated at 46 per 100, 000 inhabitants for HIV-negative individuals and 39 per 100,000 inhabitants for HIV-positive individuals respectively. However, as mentioned in the WHO TB reports for 2021,2022 and 2023, there were no national drug resistance survey or surveillance in the Republic of Congo, therefore there is limited data at hand on the prevalence and distribution of MDR-TB across the country [11, 12].
According to the TB national control program, MDR/RR-TB accounted for 5.1% of cases in the Republic of Congo in 2022, with only 37 cases of pre-XDR and two cases XDR being detected across the country [10]. This may probably reflect an underestimation of cases due to limited and insufficient testing capacity, rather than a low prevalence of MDR/RR TB in the country, as testing coverage was only 31%, with GeneXpert machines installed in just 5 out of the 12 departments [10, 13, 14].
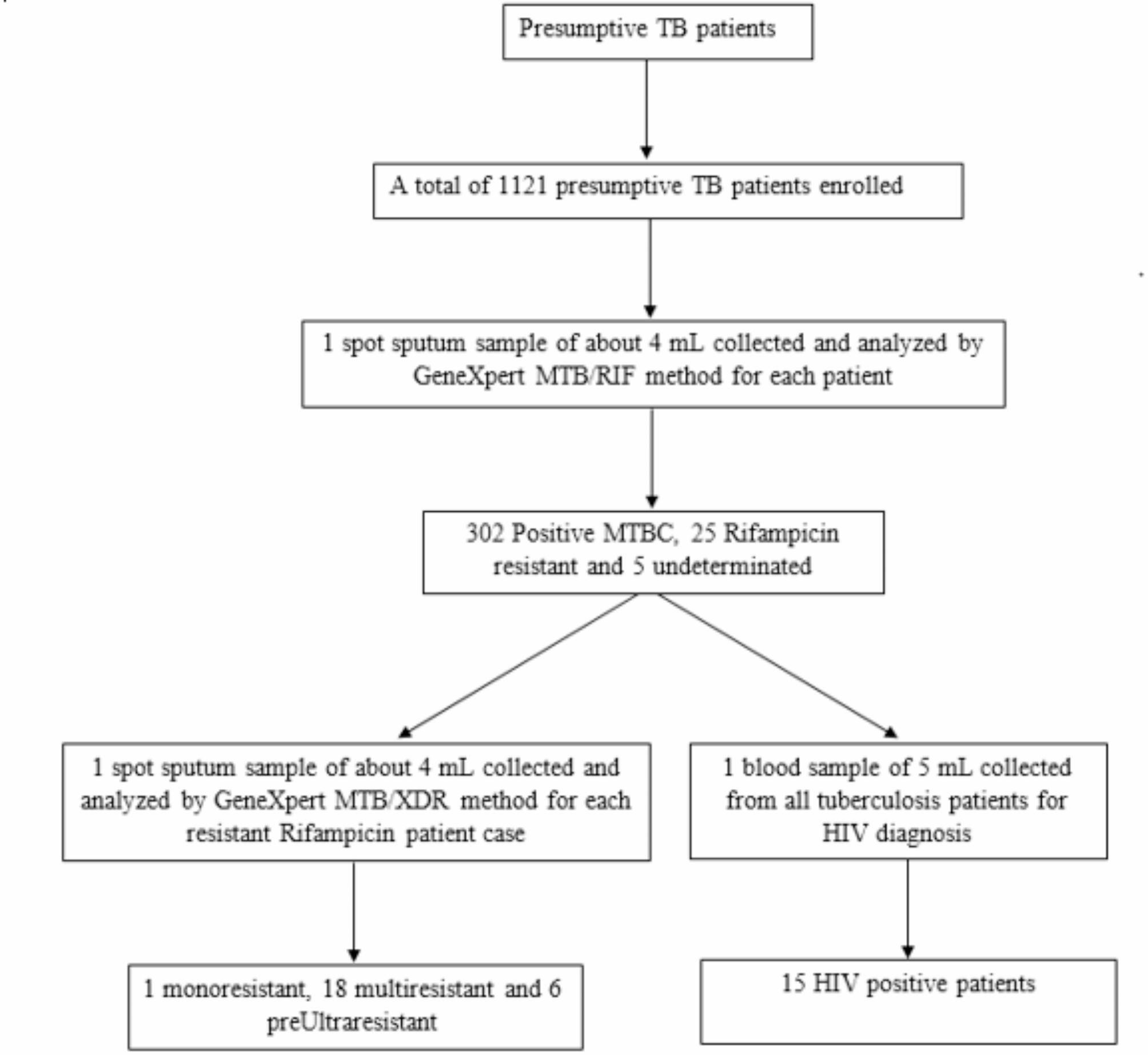
To feel this gap, a total of 23 GeneXpert (MTB) platforms were installed in 2023 in the 11/12 Departments of the Republic of Congo among which 11 (10-color Xpert MTB/XDR Xpert) used for XDR-TB resistance testing and 12 (6-color Xpert MTB/RIF), for RR-TB testing. These machines replaced AFB smear and microscopy for the initial diagnosis of all presumptive TB patients at centers equipped with Xpert, as well as the evaluation of presumptive drug resistance in samples from patients in areas without the machine Xpert (a sample transportation system is in place for these specific patients). However, despite these logistic efforts, the national coverage of MTB drug resistance testing remains low (40%) [10].
Apart from the above mentioned TB report, which are typically based on administrative records that may have limitations in consistency, accuracy, and completeness, the last study on TB drug resistance in the Republic of Congo was conducted in 2017.This study reporteda 9.8% prevalence of MDR/RR-TB in patients with no history of TB treatment [15]. Although The study faces limitation (with small samples size: 92 participants) and being conducted in peripheral screening and treatment centers (CDTs), the obtained prevalence of MDR/RR-TB was significantly higher compared to the data from the TB national control Program (5.1%). While this may not be directly comparable, it underscores the potential underestimation of MDR-TB in the country.Given these challenges, our study sought to fill this knowledge gap by investigating the drug resistance profiles of confirmed TB patients in Brazzaville, the capital and largest city of the Republic of Congo. We focused on the prevalence of MDR and XDR-TB, as well as the risk factors associated with drug-resistant TB in this setting.

Comments (0)