
Remember me

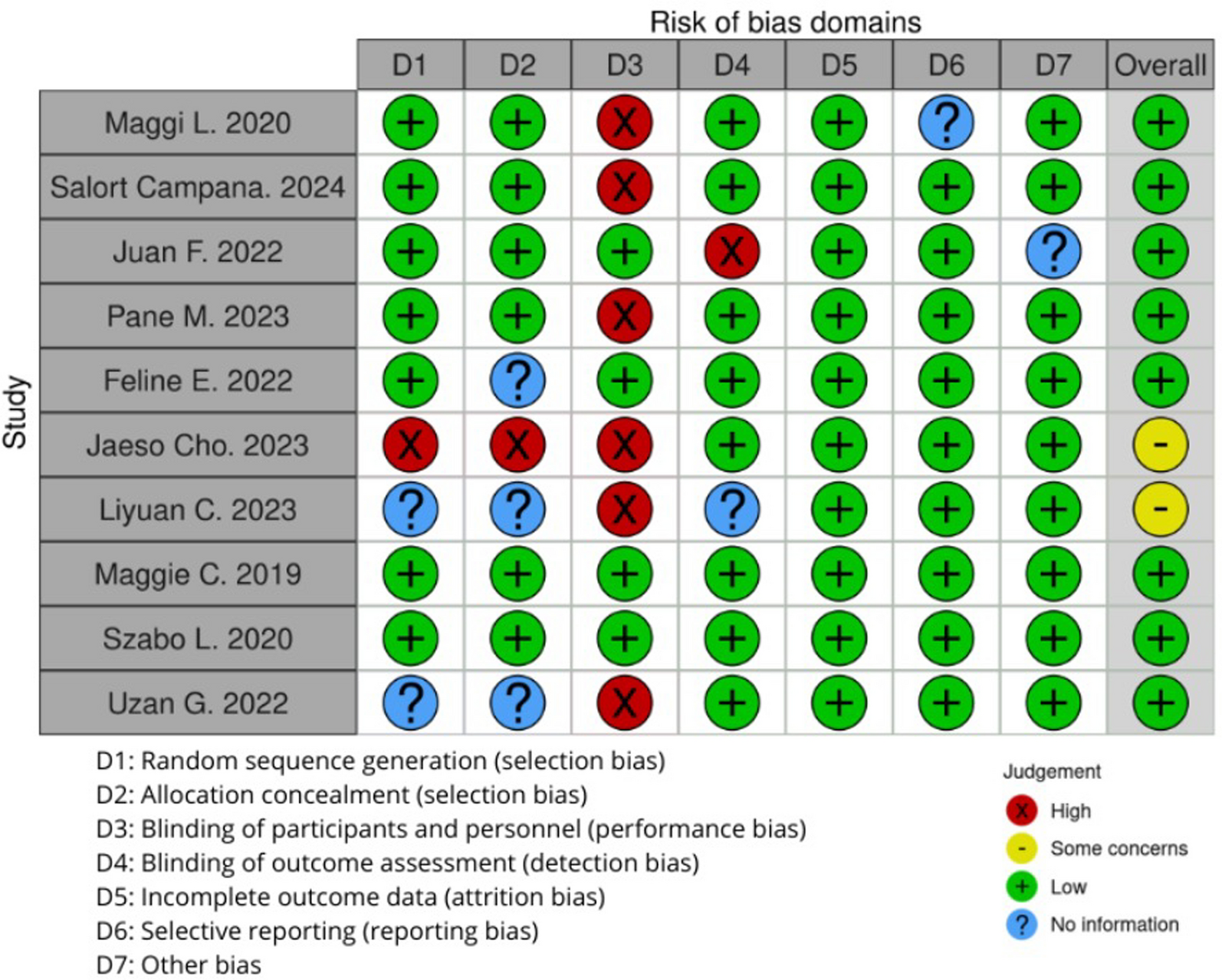


After screening the articles by two researchers, the third reviewer checked the overall quality assessment of the studies, and conflicts were resolved. A total number of 10 articles was included in the systematic review (Fig. 2).
Fig. 2
The current systematic review evaluated the effectiveness and safety of Nusinersen for the treatment of spinal muscular atrophy (SMA) based on ten studies, which included both retrospective and prospective designs, with variations in sample size, patient characteristics, and SMA type.
Cho and colleagues [3] conducted a retrospective study in Korea with 137 participants, including 21 with SMA1, 103 with SMA2, and 13 with SMA3, with a mean age ranging from 2.3 to 4.6 years. The study did not specify the number of doses. Chen and colleagues [5], in China, performed a retrospective study on 18 participants with SMA2 and SMA3, reporting a mean age of 9 ± 4.32 years for SMA2 and 11.5 ± 3.01 years for SMA3, but did not detail the number of doses. Szabó and colleagues [10], from Hungary, analyzed 54 patients in a retrospective study, including 10 with SMA1, 21 with SMA2, and 23 with SMA3, with a mean age of 0.78 (± 0.27) years. The study involved 340 Nusinersen injections. Walter and colleagues [11], in Germany, carried out a prospective study with four SMA3 patients with, a mean age of 8.00 ± 7.12 years. These patients received intrathecal loading doses of 12 mg of Nusinersen at baseline (day 1), days 14, 28, and 63, followed by maintenance doses every 4 months. Maggi and colleagues [13], in Italy, conducted a retrospective study with 116 patients (13 with SMA2 and 103 with SMA3), with a mean age of 3 years. The study used intrathecal loading doses of 12 mg Nusinersen at baseline. Salort-Campana and colleagues [14], in France, involved one patient aged 44 in a retrospective study without specifying the number of doses. Vázquez‐Costa and colleagues [15], in Spain, conducted a prospective study with 39 patients (10 with SMA2 and 29 with SMA3) and a mean age of 28.8 years. The patients received an average of six doses of Nusinersen. Pane and colleagues [16], in Italy, conducted a prospective study involving 48 patients with a mean age of 3.3 years. Among these patients, 33 received no baseline doses, 7 received one dose, and 8 received two doses. Scheijmans and colleagues [17], in the Netherlands, carried out a prospective study with 23 patients, with a mean age of 4.5 months. The study administered intrathecal loading doses at baseline (days 0, 14, 28, and 63). Uzan and colleagues [9], in Turkey, conducted a retrospective study on 13 patients with a mean age of 5 months. The study administered four loading doses of 12 mg Nusinersen at specific intervals depending on the SMA type, followed by maintenance doses every 4 months (Table 1).
Table 1 Results of the characteristics of the included studiesAnother aspect that could be noted is that the motor function of the children was shown to improve in all the studies. In [16] the study, 48 patients participated and showed significant improvement in motor function using the CHOP INTEND scale with a baseline total score of 21.0 (median 23. 0, range: 0–54) with notable changes in motor abilities after the treatment. Furthermore, it was observed that motor function improvement was evidenced across all the scales and tests with a mean increase of 20 points in HFMSE.
In [17] the study design of 23 patients, the baseline CHOP INTEND scores were reported as between 29 and 42. After treatment, 77.1% of the patients demonstrated an increase of four points or above, 14.6% showed little change, and 8.3% exhibited minor declines. The study also showed that CHOP INTEND and HINE-II scores improved in the patients with both 2 and 3 SMN2 copy numbers. In this study, no statistical differences were observed in the changes of the magnitude when comparing patients with two and three SMN2 copy numbers.
In [10] a study that involved patients with various types of SMA, the CHOP INTEND mean scores increased from baseline to 44.9 after 307 days of treatment in SMA1 patients, while SMA2 and SMA3 patients experienced significant improvements in HFMSE and other motor function measurements The 6MWT was also observed to be statistically significant at visit 5 and visit 6, although the effect size was negligible.
Uzan and colleagues [9] noted that the motor function of SMA1, SMA2, and SMA3 improved significantly after taking Nusinersen. While the SMA1 patients’ CHOP INTEND score stood at 28.5 at the first dose, it increased to 51 at the sixth dose. SMA2 patients also had a 7.2-point improvement in HFMSE. Finally, SMA3 had an improvement of 33.9 points.
In [15] a prospective study that involved SMA2 and SMA3 patients, there was a notable improvement in the motor function assessments. It was established that SMA3 sitters demonstrated higher levels of improvement than walkers and the effects accumulated over time as the overall increment in both RULM and HFMSE scores depicted (Table 2).
Table 2 Results synthesisStudy results demonstrated that survival outcomes and improvements in respiratory functions were diverse [16]. Stated that 48 patients were questioned, 14 were on spontaneous breathing, 18 were on NIV for less than 10 h per day, and 13 had tracheostomy. This suggests that although the patient’s motor function was enhanced, some were still on respiratory support after the treatment.
Scheijmans and colleagues [17] study focused on the alterations in respiratory support; some of the patients needed additional ventilation support, while others were weaned off NIV. The analysis revealed that the level of respiratory support was fluctuating, with some patients maintaining the level of support, other patients needing more ventilation, and still others improving their status. It is for this reason that most practitioners recommend that Nusinersen treatment should be done with an individual patient approach and should include frequent assessment of respiratory function.
The 180 days of treatment were described by Szabó and colleagues [10] to show moderate progression in respiratory examinations which included peak cough flows. The findings in this study noted a statistically significant increase in PCF values from baseline to 5, implying better respiratory status. Still, the effect size was moderate, indicating that the changes were not always significant and depended on the chosen indicators (Table 2).
The safety profile of Nusinersen was well-assessed in all the studies, and common side effects associated with the intrathecal injection were frequently reported and reported 45 cases of mild post-lumbar puncture syndrome and back pain, moderate side effects were observed in 10 patients including neurogenic bladder and radial neurapraxia. One of the patients needed NIV during the follow-up due to the respiratory infection, which implies that though adverse events were typically moderate, some of the patients may experience severe conditions.
Scheijmans and colleagues [17] described headache, pain, and nausea in 10/48 patients. The study pointed out that most of them were moderate despite frequent adverse events and could be controlled. None of the patients developed any manifestations of platelet or renal involvement on follow-up, supporting the safety profile of Nusinersen.
Szabó and colleagues [10] reported post-lumbar puncture headache in 10% of the injections and low backache within 48 h. of the intrathecal injection. The study indicated that such adverse events were similar to those that were reported in clinical trials and that there was no report of serious adverse events among the patients. The safety evaluation of the present study revealed that the Nusinersen application demonstrated an acceptable safety profile; the majority of reported adverse effects were associated with the procedure of the treatment.
Walter and colleagues [11] mentioned that the platelets were reducing every time the treatment was administered but would recover before the next treatment session hinting at some side effects on the platelet and renal profile but were manageable. Such side effects included thrombocytopenia and the presence of partial urinary protein which were noted to be reversible and hence no severe long-term effects were noted.
Cho and colleagues [3] stated that although some adverse effects were observed in the clinical trial, including headache, back pain, pyrexia, and discomfort, most of the treated patients did not experience severe adverse events and stayed on treatment. As for the adverse events monitoring and management, it was stated that it was critical for the safety of Nusinersen therapy. A patient also had a fever with aseptic meningitis the following day after the first injection, while another patient had an allergic skin reaction manifesting as angioedema of the lips. In addition, two patients had a rise in their intracranial pressure, suggesting that potential serious adverse events should be closely observed (Table 2).
The comparative analysis across the studies revealed the effectiveness of Nusinersen in terms of the overall findings. Motor function gains were noted with SMA3 patients and more so with the sitters compared to the walkers, as noted by Salort-Campana and colleagues [14]. This trend was also seen by Uzan and colleagues [9], where the patient had shown better motor function according to the CHOP INTEND scale and HFMSE. SMA1 patients’ average CHOP INTEND score increased by more than four points, whereas the average score for SMA2 patients rose by 7. Mean: 14.3, a 2-point increase on the HFMSE. SMA3 patients demonstrated a 33% reduced body weight compared with control patients. The beneficial effect regarding the primary outcome measure was a 9-m improvement in the 6-min walk test (6MWT) (Fig. 3).
Fig. 3
CHOP INTEND score improvements
Vázquez‐Costa and colleagues [15] study revealed that some primary adverse effects included pain and post-lumbar puncture syndrome associated with the intrathecal injection procedure. Scheijmans and colleagues [17] study supported the long-term efficacy of Nusinersen as motor function improvements remained significant, and no deterioration was observed (Fig. 4).
Fig. 4
Comments (0)