
Remember me



A female patient, 22 years old with normal body mass index (BMI = 24.9 kg/m2) presented to the neurology outpatient clinic complaining of a headache of one-month duration. This headache started as mild and then progressed till it became of moderate intensity with a visual analogue pain scale (VAS) of 6/10. This headache was mainly in the bifrontal and bitemporal areas. The pain was dull-aching and continuous day and night. It did not wake her up from sleep but started to interfere with her daily activities one week before the consultation. The pain increased significantly in the laydown position and slightly decreased in the upright position. The headache was associated with blurred vision bilaterally, but there was no transient visual obscuration. There was no nausea, vomiting, photophobia or phonophobia. There was no history of other neurological problems. She is married, but not on hormonal contraceptive methods.
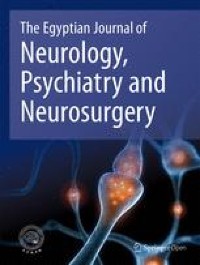
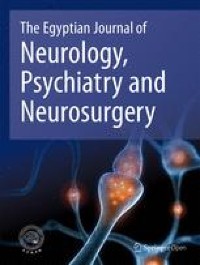
The general and neurological examination was normal except for grade II papilledema bilaterally. She underwent an MRI head which revealed CLOCC as a rounded lesion in the splenium of the CC with restricted diffusion. The MRV revealed segmental mild stenotic lesions of the transverse veinous sinuses bilaterally (Fig. 1A, C). A lumbar puncture (LP) was performed, and the CSF was clear with an opening pressure of 26 cmH2O. Blood tests including thyroid function, Liver function, kidney function and blood picture were normal. The CSF analysis was normal for protein and glucose and negative for virology PCR and bacteriology culture. The lymphocyte count was elevated (Table 1). The patient was diagnosed with IIH and commenced acetazolamide 500mg bd in addition to paracetamol for pain relief.
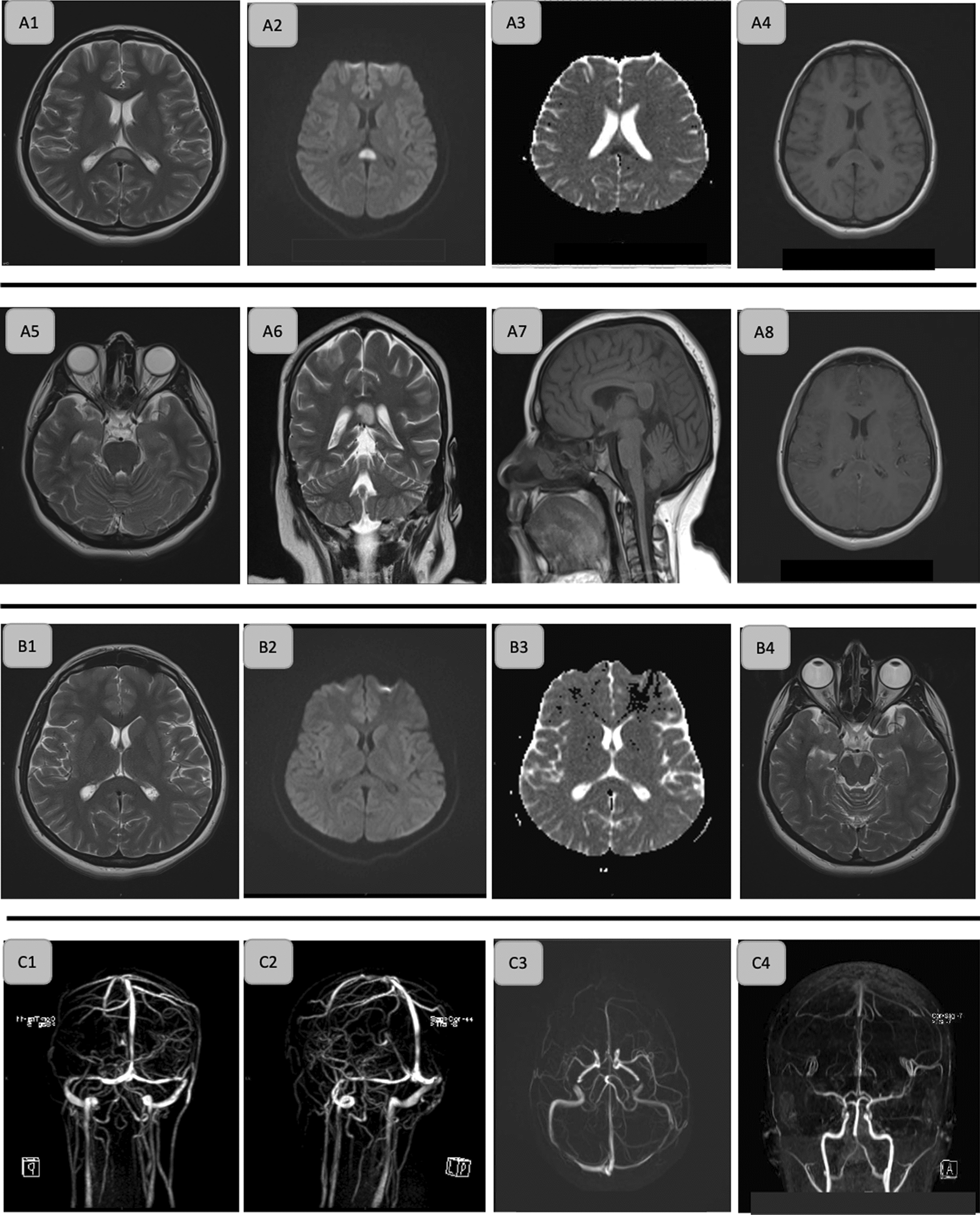
Fig. 1
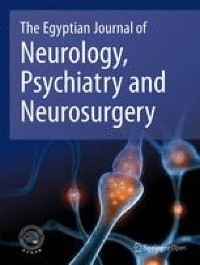
The MRI brain and MRV head of the patient. A, initial MRI head at the time of presentation illustrating cytotoxic lesion of corpus callosum as a rounded lesion in the splenium of the corpus callosum with restricted diffusion There were slightly prominent peri-optic CSF spaces and normal Sella: (A1: T2 axial, A2: DWI axial, A3: ADC axial, A4: T1 axial without contrast, A5: T2 axial optic nerve level, A6: T2 coronal, A7: T1 sagittal, A8: T1 axial with contrast). B, follow up MRI head illustrating complete disappearance of the cytotoxic lesion in the corpus callosum and improvement the peri-optic CSF spaces: (B1: T2 axial, B2: DWI axial, B3: ADC, B4: T2 axial optic nerve level). C, 3-D MRV and MRA showed segmental mild stenotic lesions of the transverse veinous sinuses bilaterally
Table 1 Laboratory investigations including CSF analysisAround 6 weeks later, the patient attended for review with markedly improved headache (VAS = 2/10). The follow-up MRI at that time revealed a complete disappearance of the CLOCC with an apparent normal study (Fig. 1B). The Fundus examination revealed resolved optic disc bilaterally. The patient continued taking acetazolamide 500mg bd.
CLOCC term was proposed by Starkey and colleagues in 2017 who explained a callosal lesion that was not restricted to the splenium, not usually reversible, and could be associated with severe complications [2]. Earlier studies used the terms “reversible splenial lesion syndrome” (RESLES) or “mild encephalopathy with a reversible lesion in the splenium” (MERS) [4]. Some studies sub-classified it further into callosal-restricted small lesions and large expandable lesions [8]. Here, we reported a case of IIH with a reversible small restricted splenial lesion.
The aetiology of this cytotoxic reversible lesion is still unclear; however, the release of cytokines like interleukins 1 (IL1), IL 6, and tumour necrosis factor-alpha (TNF-α) could cause microglial activation, increase glutamate synthesis and secretion, mitochondrial dysfunction, and water influx into neural and glial cells causing cytotoxic oedema [3]. This could explain the increased level of mononuclear cells in the CSF. The splenium is mostly affected as it has a double blood supply and high sensitivity to glutamate [3]. Many triggers can cause this cascade of actions including anti-seizure medications, viral encephalitis, malignancies, metabolic disturbances, altitude sickness and migraine with aura [2].
A similar published case reported CLOCC in a patient with a new daily persistent headache after stoppage of acetazolamide followed by volume decrease with LP [9]. This indicated that the rapid alteration in the CSF pressure or volume could trigger the cascade of cytokines release causing CLOCC. This was supported by a study performed by Dhungana and colleagues which revealed the presence of these cytokines in the CSF of patients with IIH [7]. Our case was different as it illustrated that the CLOCC appeared after idiopathic increase the CSF pressure not stopping the medication. Therefore, our case is considered the first case addressing this. Another report revealed that corrective surgery to repair the CSF leakage was associated with increased the serum levels of IL-6, IL-10 and TNF-α [10]. Despite this was hypothesized to be due to the surgery, the CSF alteration could play a role itself.
Comments (0)