It is evident from the studies in the literature that diagnostic delay in CH is not confined to a geographical area [6, 9]. Although some countries had less delay than others, delays in the diagnosis were recorded in multiple countries in Europe, the United States of America (USA) and Japan. One possible reason could be limited knowledge about the characteristics of CH across countries [6]. Misdiagnosis invariably leads to mismanagement. In CH, due to the severity of the symptoms, patients desperately seek the opinion of several specialists until the symptoms are alleviated. It is possible that some specialists feel the need to offer invasive procedures in an attempt to provide some form of relief, even if the chance of success is small [10].
In our study, more than half of the participants did not hear about CH before, despite on average 15 years of clinical experience. Moreover, in our study, 63.6% of neurosurgeons and 20.7% of internists started treatment for CH without referral to specialized headache clinics. Patients consulted different physicians, but in most cases, their CH was first diagnosed by neurologists or headache centre specialists. The physicians most frequently consulted at the onset of disease, after neurologists, were primary care physicians, ENT specialists, dentists and various non-medical therapists [11]. These professionals may be less familiar with CH, and this might indeed help to explain the diagnostic delays reported [11]. In literature, about one third of the patients were at some time in the diagnostic process referred to dentists or ENT specialists, or both. CH is comparatively often mistaken for sinusitis or a dental disorder [11]. Most of the patients were diagnosed by neurologists or primary care physicians [11]. Therapeutic errors in CH can be avoided when appropriate drugs are available; these should be prescribed, according to the current international guidelines, by headache specialists or general neurologists, who are, in fact, usually the ones who first diagnose the disease [12, 13]. Vikelis and Rapoport [14] showed that nearly two-thirds of their Greek patients (63.5%) consulted a general practitioner or an internist; around one-third an ENT specialist, ophthalmologist or dentist, and a small proportion (8.5%) a neurosurgeon. In the same study, 40% of the patients were seen by neurologists who missed the diagnosis.
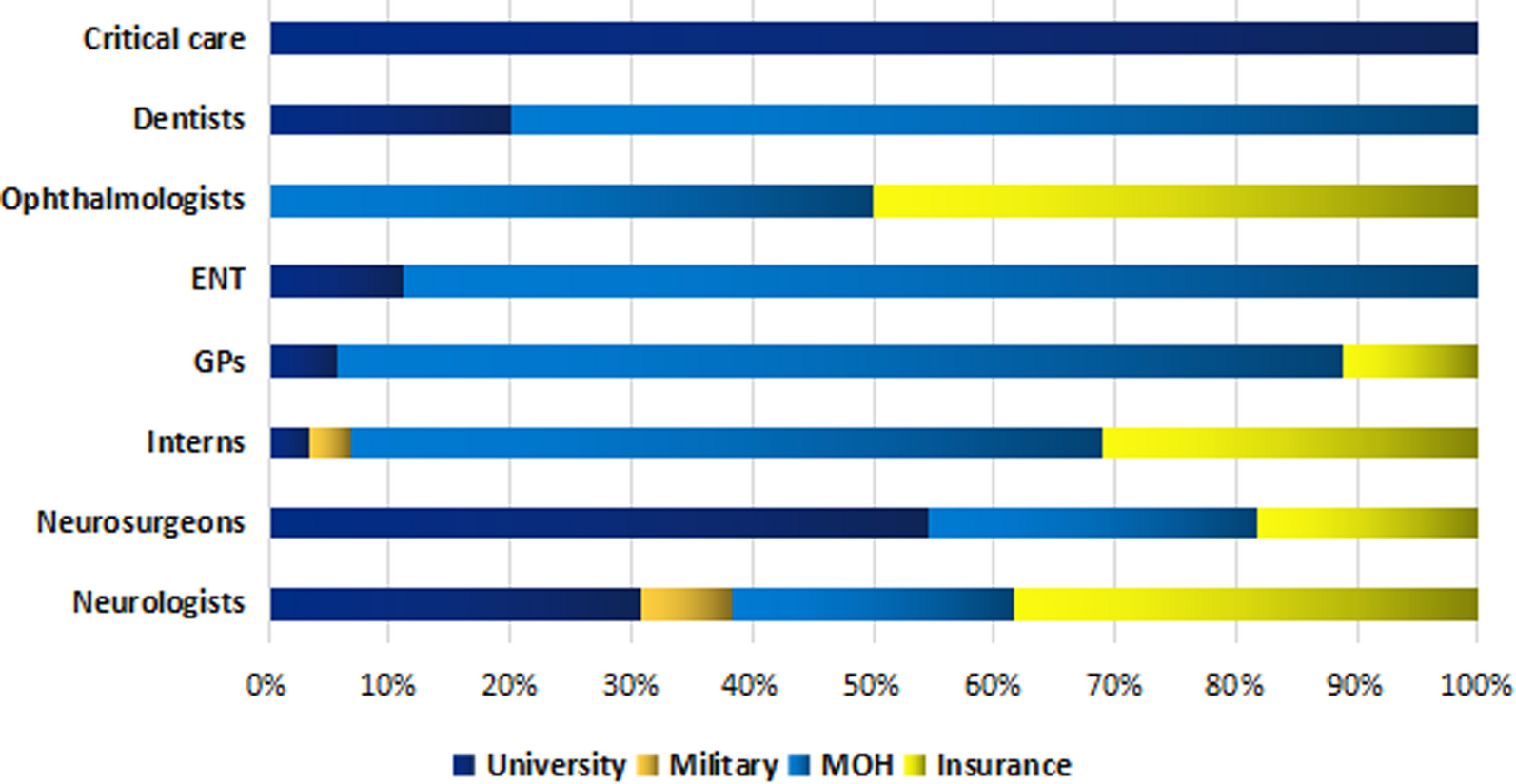
Although no controlled studies are available for topiramate to be used as preventive medicine in patients with CH [10], most neurosurgeons (81.8%), ENT specialist (55.6%) and internists (41.4%) use it as preventive therapy for CH in our study. In contrast, 11 of the 13 neurologists recruited (84.6%) preferred verapamil, which is the only drug approved after controlled trials [10]. Migraine preventives, such as propranolol and pizotifen, are generally accepted to be ineffective, but are widely prescribed for cluster headaches [15]. In our study, however, propranolol was reported by 4.3% of the sample to be the preventive medicine for CH. Kim et al. [16] confirmed the delay and errors in the diagnosis of CH, and pointed to clinical significance of diagnostic criteria and headache education in reducing the delayed diagnosis of CH. Although some neurologists offer non-evidence-based CH treatments [10]; cluster headache should be managed by neurologists to minimize the patient’s disability and suffering [13].
Inhalation of 100% oxygen at a rate of at least 12 L/min given through a non-rebreathing mask and reservoir bag is rapidly effective in relieving pain in most sufferers [17]. In spite of the absence of subcutaneous or nasal triptans in Egypt, only two neurologists (15.4%) prescribed high-flow oxygen therapy as abortive treatment. This adds more suffering to the patients. This is much lower use of oxygen therapy than in other countries. For instance, In Italy, Moldova, Ukraine and Bulgaria oxygen was prescribed in 45 patients (22%) and triptans in 108 patients (52.7%). Although some neurologists offer non-evidence-based CH treatments [10].
Byung-Su Kim and colleagues [16] highlighted the significance of awareness about the clinical criteria and disease burden for reducing the diagnostic delay of CH. In our study, only 24 (26.1%) (13 neurologists, six neurosurgeon, and five interns) out of 92 clinicians were aware about the international diagnostic criteria and guidelines of treatment. In Italy and Eastern Europe, there were still some patients (no. = 34, 16.6%) who were receiving non-guideline-recommended symptomatic treatments [2], while 12 patients (8.3%) were not prescribed any symptomatic treatment [10].
Cluster headache is associated with an increased suicidality during attacks and within the active cluster period. Short and long-term disease burden from CH as well as depressive symptoms contribute to the ictal and interictal suicidality in CH patients [18]. Even though, only 5 (5.4%) physicians assessed depression and suicidality in patients with CH; three of them were neurologists.
Though cluster headache is generally included in undergraduate teaching courses in Alexandria university and the different Egyptian universities, approximately one fourth only of the participants recalled they received undergraduate information about the disease. Therefore, it seems that undergraduate teaching is not adequate. Educational programs are highly recommended to target postgraduate physicians who commonly deal with headaches in the community.




Comments (0)