Recently, with the advancements in beauty repair technology, the aesthetic requirements of people have increased. The first part affected by aging is the periorbital region, and periorbital wrinkles are a problem faced by many middle-aged women. The periorbital skin lacks collagen, and the secretion of dermal sebaceous and sweat glands decreases. After the periorbital skin loses the support of the adipose tissue, the skin gradually becomes loose and rough [3]. With the popularization of laser skin replacement technology, ablative CO2 lasers have become the first-line treatment method for white facial skin replacement. However, their further application is hindered by their long healing time, scarring, and postinflammatory pigmentation. To overcome the risk of complications, Manstein et al. proposed the theory of fractional photothermolysis (FP) for the first time in 2003 [16], and the designed CO2 AFL has been widely used in clinics. The use of CO2 AFL for the treatment of static periorbital wrinkles has been shown to be effective. Karsai used CO2 AFL to treat periorbital rhytides, and the wrinkle depth and Fitzpatrick score were reduced by approximately 20% and 10% [11]. Our study showed that the investigators’ and patients’ visual evaluations demonstrated a consistent effectiveness rate of 68.2%.
Hantash et al. first reported the photothermal effects of an ablative CO2 fractional laser on human skin in vitro and found that, in an ablative microarray, the center of the microthermal zone (MTZ) penetrated deep into the dermis, surrounding it with a circular zone of tissue coagulation [17]. This effectively promotes coagulation and hemostasis, while circular coagulation and tightening of collagen results in multiple small contractions, contributing to immediate, visible skin tightening, as well as long-term sustained tightening. In the same year, they also reported pathological changes following the application of an ablative CO2 fractional laser to the human forearm skin [18]. The early response protein HSP72 was significantly upregulated 48 h after treatment, peaking at 2–7 days; HSP47 exhibited delayed expression, appearing at 7 days and lasting for at least 3 months, with diffuse expression throughout both the epidermis and dermis. Dermal remodeling extends well beyond the immediate MTZ area, which is particularly beneficial in treating static wrinkles that are typically caused by dermal atrophy and loss of skin elasticity. This pathological study further confirmed the intrinsic mechanisms underlying the clinical efficacy of CO2 fractional laser.
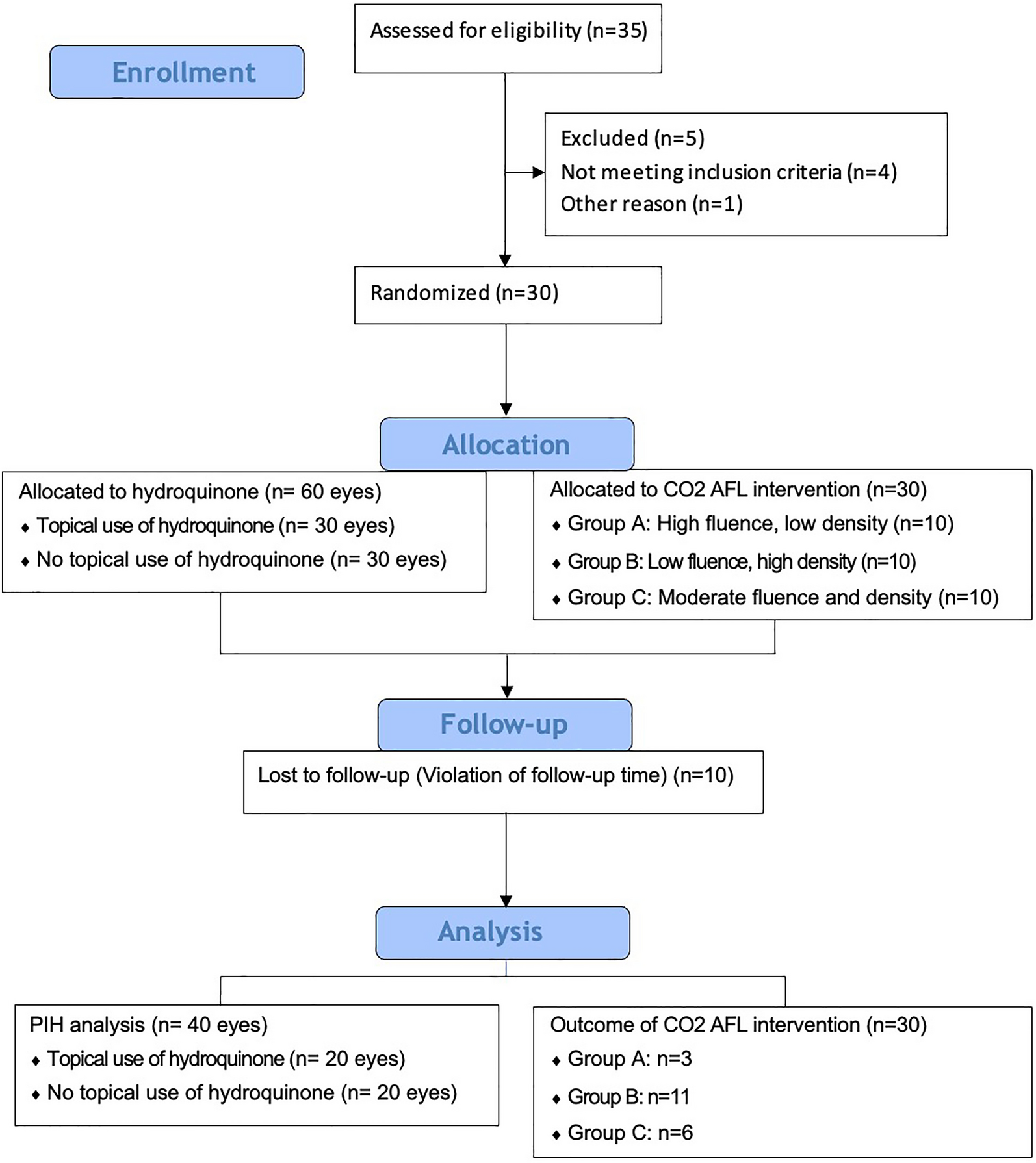
Our findings suggest that low-energy, high-density CO2 AFL parameters (10‒12.5 mJ, 15% density) are the most effective for treating static periorbital wrinkles, with patients continuing to show reductions even at 6 months post-treatment. The rationale behind using low energy with high density lies in achieving an optimal balance between efficacy and minimizing adverse effects, such as prolonged erythema and PIH. Notably, in our study, the energy of 10‒12.5 mJ was set as a relatively low grouping. However, the depth that this energy can penetrate is 0.3‒0.4 mm, and the depth of the whole skin layer of the lower eyelid is only approximately 0.5 mm, so it is enough to effectively stimulate the collagen production of the dermis [19]. However, the high-energy, low-density and medium-energy, medium-density groups were not as effective. There is a lack of relevant evidence on how to select the coverage rate when using fractional CO2 laser for skin rejuvenation in Asian individuals. Typically, coverage rates reported for white populations range from 20–45% or even higher [20]. Nevertheless, such high coverage rates pose a significantly higher risk of PIH for Asian individuals with Fitzpatrick skin types III–V. Therefore, the maximum coverage rate used in this study was 15%, which has been found to strike a good balance between efficacy and safety. Using low-energy levels reduces the depth of penetration and thermal damage, decreasing the likelihood of PIH, whereas using a high density ensures sufficient coverage of the treatment area, leading to uniform collagen stimulation and skin resurfacing.
The long-term effectiveness observed at 6 months post-treatment can be attributed to the extended period required for collagen remodeling and skin maturation. Collagenesis is a gradual process that continues for several months after laser therapy, and the cumulative effects of two CO2 AFL sessions likely contributed to sustained improvements in wrinkle reduction. This prolonged effect has been corroborated by other studies, such as that by Ross et al., who found that CO2 induces collagen remodeling that persists for several months after post-treatment [21]. Ross et al. conducted a CO2 laser study on the periorbital and perioral regions in 13 patients. Biopsies were obtained before treatment, immediately after treatment, and either 3 or 6 months after treatment to evaluate the degree of fibroplasia. Histologic examination demonstrated that the fibroplasia thicknesses after 3 and 6 months were 63 ± 41 um and 56 ± 45 um, respectively.
PIH is a common complication in darker skin types, particularly in East Asian patients, following CO2 AFL treatments. Hydroquinone remains the gold standard for the treatment of PIH. It is a phenolic compound that inhibits tyrosinase, thereby reducing the conversion of dihydroxyphenylalanine (DOPA) to melanin [22]. Studies focusing on the prevention of PIH following CO2 laser resurfacing have suggested that the use of sunscreen or hydroquinone combinations is a critical preventive strategy [23]. However, the efficacy of only hydroquinone in preventing PIH following CO2 laser treatment remains unclear. In the largest clinical trial conducted, 100 participants were randomly assigned to receive pre-treatment on the face with either 10% glycolic acid cream, 4% hydroquinone cream, or 0.025% tretinoin cream, or no pretreatment for a maximum duration of 2 weeks before undergoing laser therapy. Analysis based on clinical photographs revealed no statistically significant differences in the incidence of PIH among the various treatment groups[24]. One of the critical findings of our study was the significant reduction in PIH when hydroquinone was applied before and after treatment (chi-squared test, p = 0.02). This finding highlights hydroquinone as an essential component of pre- and post-laser care in patients with darker skin tones. It should be noted that long-term use of hydroquinone and its potential side effects include skin irritation, exogenous ochronosis, carcinogenicity concerns, rebound hyperpigmentation, photosensitivity, and regulatory and safety precautions. However, short-term, supervised application at the lowest effective concentration, coupled with sun protection and periodic breaks, is critical to balancing efficacy and safety. Patients should be informed of risks and alternatives, particularly those with darker skin or requiring prolonged treatment.
This study had a limitation. The small sample size of this study may have reduced its statistical efficacy. It is necessary to include a larger number of patients and conduct a multicenter study to further confirm the research results. Indeed, a 6-month follow-up period is not exceptionally long. However, for conditions such as dynamic wrinkles, which are relatively easier to address by botulinum toxin, therapeutic effects are typically maintained for only 4–6 months. The causes of static wrinkles are multifaceted, involving not only atrophic factors due to collagen loss but also facial mimetic muscle movement, photoaging, gravitational effects, facial distortion during sleep, and others. Given that the improvement persisted for 6 months after just two sessions of treatment, patients were already highly satisfied with the outcomes. Therefore, we did not conduct follow-up longer than 6 months.



Comments (0)