
Remember me


The study was conducted from March 2023 to August 2023 at Servei Central de Suport a la Investigació Experimental Universitat Valencia, Valencia, Spain, according to the general conditions of the center established for research studies involving human cell lines.
Cell Viability AssayCell viability was assessed using the MTT reduction assay to evaluate the cytotoxicity of the moisturizer on normal human epidermal melanocytes M2. Cells were exposed to various concentrations of the moisturizer (0.0003, 0.001, 0.003, 0.01, 0.03, 0.1, 0.3, or 1% v/v) for 5 days, with daily medium changes. Controls included the pre-treatment status of cells to assess the cytotoxic, cytostatic, and proliferative effects of the tested sample (Control 0h), untreated cells (Control), and empty wells filled with product dilutions to control for non-specific MTT reduction. After incubation, absorbance was measured at 570 nm to assess cell viability. Full details of the cell viability assay are provided in the Supplementary Material.
Melanin Content QuantificationMelanin accumulation was quantified following daily sequential ultraviolet-A (UVA) exposure, which was delivered in three steps: 20 min on day 1, 30 min on day 2, and 40 min on day 3, delivering a total dose of 16 J/cm2. During this period, cells were incubated with treatment at sub-cytotoxic concentrations of 0.001% and 0.0001%, with daily medium changes. After the 3 days of UVA irradiation, fresh medium was added, and the cells were incubated for an additional 2 days to allow for melanin accumulation in the UVA-exposed cells. Control groups included untreated cells with no additional components (Control) and untreated cells exposed to daily UVA irradiation (Control + UVA). Melanin content was then extracted and quantified by measuring absorbance at 405 nm. The full procedure for melanin quantification is provided in the Supplementary Material.
Statistical AnalysesStatistical analyses were performed with the GraphPad Prism V9 software (Insightful Science and Dotmatics, Boston, MA, USA). Data were analyzed by one-way analysis of variance with Dunnett’s multiple comparison test. All statistical analyses employed a significance level of p < 0.05. For the MTT assay, data were normalized versus the untreated control and are expressed as a percentage (%). For melanin quantification, both viability and melanin absorbance values were normalized against UVA-exposed cells (Control + UVA). Normalized data were represented in bar graphs as mean ± standard error of the mean (SEM).
In Vivo MethodsEthical approval was granted by Dermaclaim Lab S.L., Spain. The study adhered to the principles of Good Clinical Practice and the Declaration of Helsinki and its subsequent amendments. Prior to enrollment in the study, written informed consent was obtained from all participants for the participation and for the publication and use of all participants’ images.
Study DesignThe single-center, controlled clinical study was conducted between March and June 2023 at Dermaclaim Lab S.L., Valencia, Spain. The study adhered to the principles of Good Clinical Practice and the Declaration of Helsinki and its subsequent amendments. The study was performed following UNE-EN-ISO 9001/2015 Quality Management System guidelines (reference code, EC-10984/22).
Study PopulationThirty-three females aged 30–55 years, with non-sensitive skin of various types (normal, combination, oily), and spanning Fitzpatrick phototypes I–VI, provided informed consent to participate in the study. All participants had moderate-to-severe facial hyperpigmentation spots, ranging from grades 2 to 4 according to the Eiben-Nielson photonumeric scale [25]. Participants undergoing medical treatments that could interfere with the study, as well as those who had received esthetic treatments on the face within 3 months before the study commencement, were excluded.
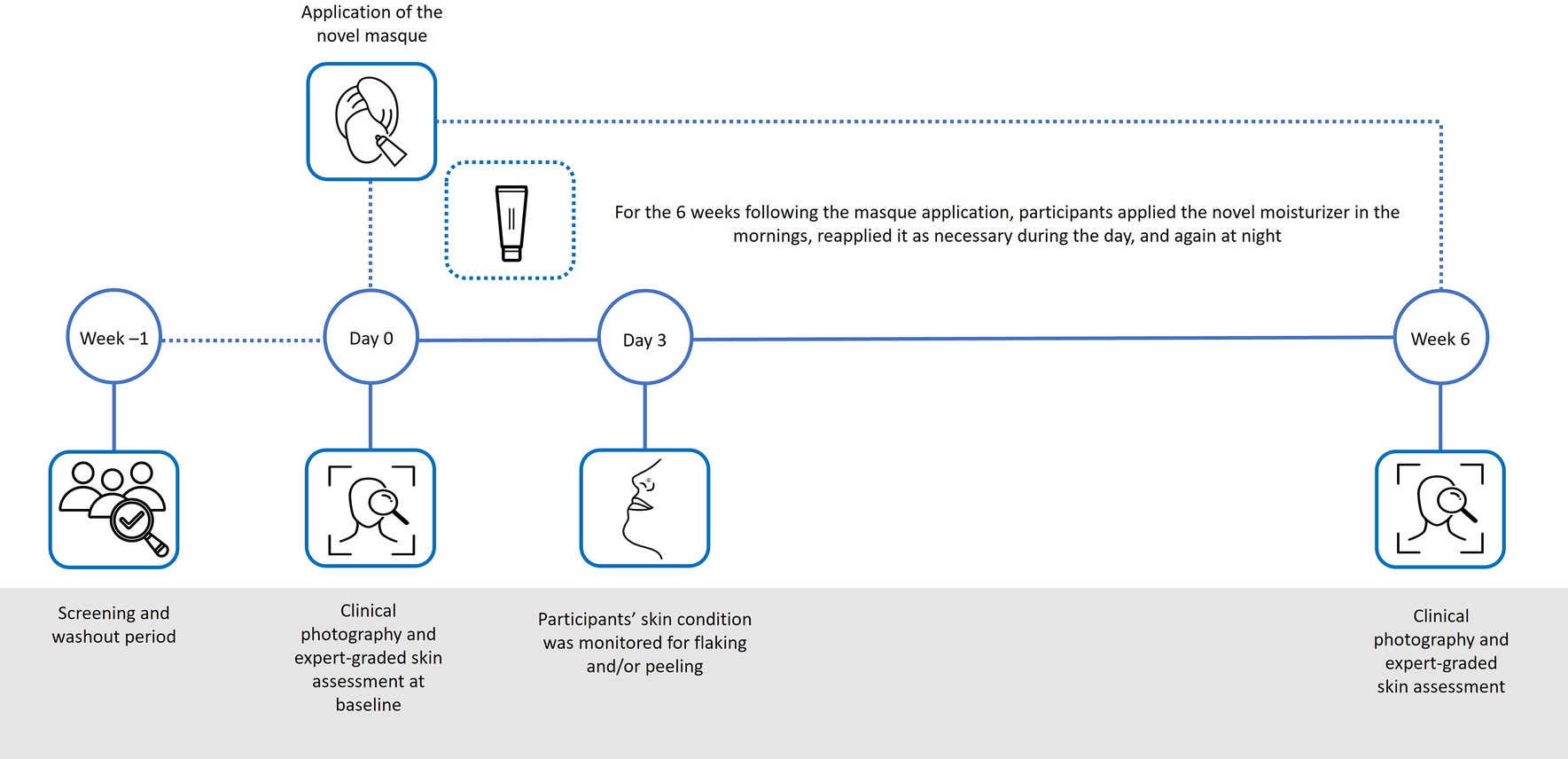
ProcedureThe study was conducted for 6 weeks, with four visits in total (Fig. 1).
Fig. 1
Timeline and treatment schedule
One week before the first study visit, as part of the 2-week washout period, participants were instructed to follow a specific morning skincare routine: cleansing, moisturizing, and applying sunscreen to the face. Make-up could be applied after 5 min, but no other creams or serums were permitted. If make-up was applied, it had to be removed before participants’ evening skin care routine, which comprised cleansing and moisturizing the face. Participants arrived at the test site and spent 15 min acclimating to the clinic environment, where the temperature was maintained at 23 ± 1 °C and the relative humidity at 45 ± 10%, before baseline assessments. Following this, a licensed esthetician applied the novel masque evenly to the face, leaving it on for 3 h before rinsing it off with cold or lukewarm water, avoiding rubbing the skin. A toner was then applied and could be reapplied as needed to alleviate sensations of tightness, dryness, or itching. The following day, participants exclusively used the toner on their face and were told to avoid sun exposure. Participants visited the test site on day 3, where their skin condition was monitored for flaking and peeling by the Clinical Project Manager of the research center or by a qualified and experienced technician under their supervision. For the 6 weeks post-treatment, participants followed a skincare routine. In the mornings, they gently cleansed the skin and applied a toner (up until week 1). After applying the toner at week 1 and directly after cleansing from weeks 2 to 6, participants applied the novel moisturizer, which could be reapplied once more during the day if the skin felt very dry or irritated. After applying the moisturizer, participants were advised to wait a few minutes before applying sunscreen to the face and at least 5 min before applying make-up unless the skin was irritated. In such cases, it was recommended to avoid make-up entirely until the skin recovered. For the nightly routine, participants were instructed to remove make-up if applicable, gently cleanse the face, and apply the novel moisturizer.
OutcomesChanges in skin condition and clinical photography were assessed at baseline and week 6 by the Clinical Project Manager or by the responsible technician under their supervision, both of whom were trained professionals experienced in clinical evaluations. High-resolution macroscopic pictures of the skin were obtained using a camera (Nikon D5600) installed in the HeadScan Bench Light Face.
Skin parameters, including dark spots (total number, area, perimeter, skin homogeneity, and skin contrast), tone (CieL* for lightness, CieA* for green–red, CieB* for blue–yellow in the CIELAB color space, and Individual Typology Angle), and brightness (specular brightness, diffuse brightness, skin lightness, and global brightness) were recorded from the region of interest (ROI) on each side of the participant’s face. ROIs were first defined at the starting time for the chosen subject and then automatically replicated in the same position across all images. Notably, ROI sizes remained constant for reliable quantifications across different kinetics times for the same subject. FrameScan V4 software was used to quantitatively analyze digital 2D photographic images for colorimetric and morphologic characteristics.
Skin surface roughness of the nose–cheek area on both sides of the face was evaluated using the AEVA-HE V4 3D skin topography system, a high-resolution 3D scanning sensor used for measuring skin amplitude, roughness, and volume. Various parameters were analyzed to characterize skin surface roughness, including Sa (the average value of all height points), St (the maximum height deviation on the surface, peak to peak), Sr (the ratio of the real developed area to the apparent area), Sq (the standard deviation of the height points), and Stm (the average of the 25 local peak-to-peak values).
Dark spots, lack of radiance, and uneven skin tone were subjectively assessed by clinical expert evaluation (CEE). Dark spots were evaluated according to the Scientific Assessment Scale of Skin Quality, a 5-point ordinal scale (“0 = no pigmentation” to “4 = very severe pigmentation”) for skin pigmentation [25]. Lack of radiance and uneven skin tone were evaluated according to the 10-point Modified Griffiths Scale (“0 = none” to “9 = severe”)[26].
At the end of the treatment period, participants completed a questionnaire to evaluate the subjective efficacy of the innovative peeling system and their satisfaction with the treatment according to a 5-point ordinal scale (“1 = strongly disagree” to “5 = strongly agree”). The questionnaire was designed in collaboration with the sponsor.
Safety was monitored throughout the study. A visual examination of the experimental area was conducted by the responsible technician before and after treatment. Participants were instructed to report any adverse events observed or sensations of discomfort experienced following the use of the innovative peeling system to the technician overseeing the study.
Statistical AnalysesStatistical analyses were performed with the GraphPad Prism V9 software (Insightful Science and Dotmatics, Boston, MA, USA). Analyses included all participants who received treatment and completed the study (per protocol), and data were analyzed by applying the paired Student’s t-test. Individual post-treatment values for dark spots, skin brightness, tone, and surface roughness were normalized against baseline measurements for the entire group to account for baseline variability among participants and ensure accurate interpretation of treatment effects. Results were expressed as a percentage relative to baseline values and the mean ± SEM was calculated. To maintain the integrity of subjective evaluations and avoid potential misinterpretation, CEE scores were not normalized against baseline measurements and are expressed as mean ± SEM. All statistical analyses employed a significance level of p < 0.05, with 95% confidence intervals (CIs) reported where available.
Comments (0)