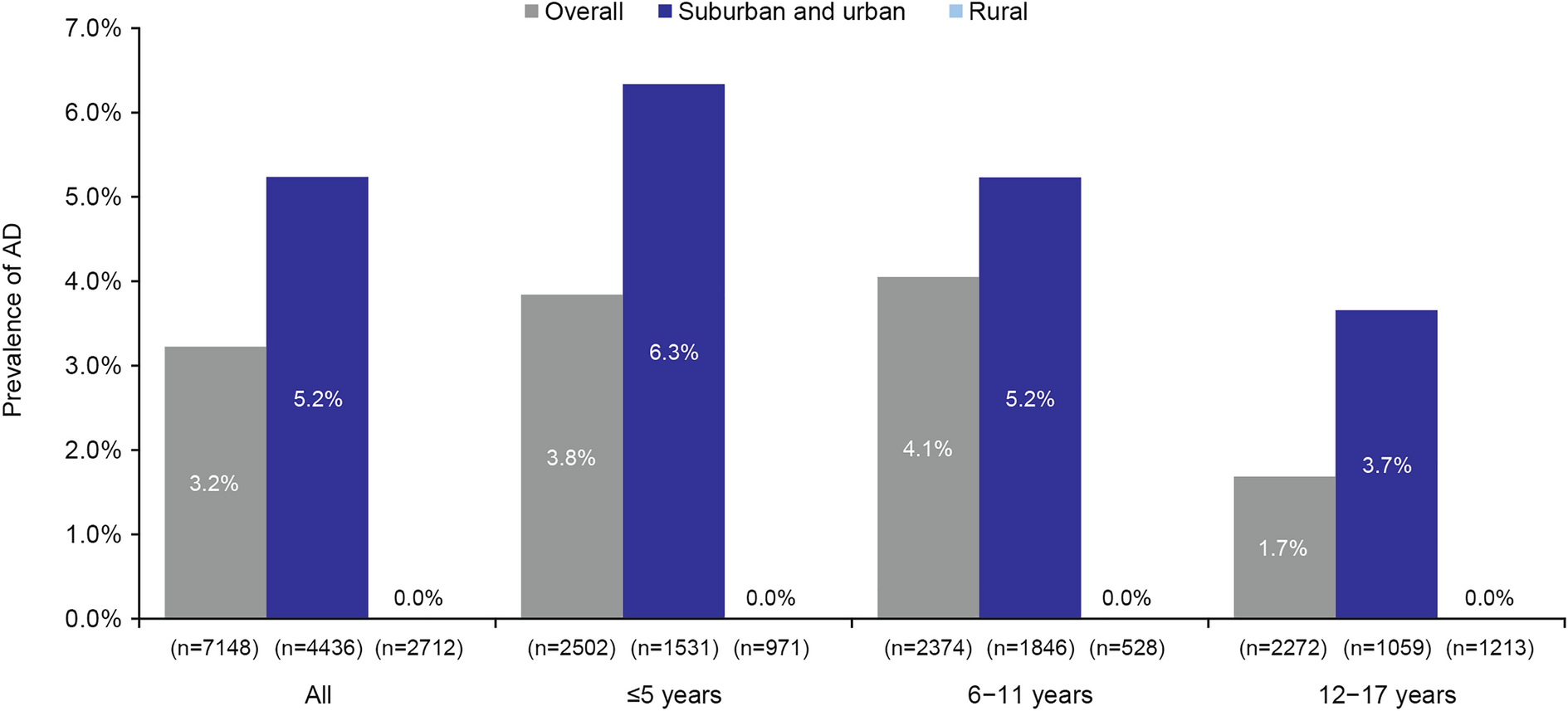
This survey demonstrated that approximately 3% of the pediatric population in China were affected by AD, and those patients experience a substantial disease burden across multiple domains, including type 2 inflammatory comorbidities and AD-related symptoms, such as itch, skin pain, and sleep disturbance. Additionally, although sample sizes were small, dermatology PRO tools (the IDQoL and the CDLQI) suggested that the presence of AD was associated with substantial impact on HRQoL and that this impact was greater in patients with moderate versus mild AD (too few patients with severe AD completed the IDQoL and CDLQI to enable meaningful analysis).
These data extend previous reports across multiple geographical locations from the EPI-CARE study. Prevalence estimates in China were generally lower than those seen in corresponding EPI-CARE studies in other geographical regions, despite comparable methodology; in a previous multinational report from the EPI-CARE study, only Israel (2.7% in children aged 0.5–17 years) had a lower prevalence of pediatric AD [6]. The reason for such wide geographical variation in AD prevalence is currently unclear but is likely to relate to a combination of ethnic, racial, and/or socioeconomic factors [11]. These results are also broadly in line with prior assessments of pediatric AD in China. A large-scale multicenter face-to-face dermatology assessment reported a prevalence of 4.8–12.9% in children aged 1–7 years [12]. Similarly, in a 2010 prior cross-sectional study in preschool children aged 3–6 years in Shanghai, China, the prevalence of AD diagnosed according to UK working group criteria [13] was 8.3% [14]. The slightly lower AD prevalence observed in our study may be attributable to the use of ISAAC criteria and to our conservative AD definition, whereby AD cases were also required to have a self-reported or parent-reported confirmation of a physician diagnosis of AD. Indeed, although we employed a dual-factor identification (both self-reported ISAAC criteria and self-reported or parent-reported physician-confirmed diagnosis) in this study, self/parent-reported physician-confirmed AD rates were much higher than ISAAC-based AD rates, which aligns with previous studies. The studies reported by Guo et al. (2016) and Xu et al. (2012) also reported that the prevalence of pediatric AD was higher in urban than in rural areas in China. Xu et al. (2012) noted industrial manufacturing, pollution, exposure to animals, maternal age, overcrowding in an apartment, differences in diet (e.g., processed versus fresh food), socioeconomic factors, and time spent indoors as potential factors leading to higher pediatric AD prevalence in urban areas. The association between AD prevalence and urbanization has also been observed in other countries; a systematic review of AD prevalence in children and adolescents reported that this link was particularly strong in developing countries [15]. Potential contributing factors noted in the systematic review broadly match those highlighted in the Xu 2012 study, but additional factors mentioned were water intake (e.g., spring versus chlorinated water), increased vehicular traffic, and differences in climate.
The majority of patients across all age groups assessed experienced mild or moderate AD, which is in line with previous reports in adult AD populations [4] and were broadly comparable with scores reported for these age groups in other geographical locations [6]. We assessed severity primarily by PGA, which we assume to represent a more precise and holistic measure of severity than other symptom-based measures, such as POEM. Our sensitivity analysis using POEM to assess severity demonstrated similar findings to PGA. The observations that the prevalence of severe AD increases with age, with a parallel decrease in mild AD, may indicate a progression of severity in patients with AD (i.e., patients with mild AD at a young age may develop more severe AD by the time they reach 11–17 years of age). Similarly, another population-based study from the UK also reported a decrease in the prevalence of mild AD concurrent with an apparent increase in the prevalence of severe AD [16]. Similarly, the proportion of patients reporting more than one comorbidity and also the rates of specific type 2 inflammatory comorbidities, such as food allergies and allergic rhinitis, appeared to be more frequently reported with increasing age. The link between AD and allergic rhinitis has previously been demonstrated [17, 18]. Taken collectively, these observations of increasing severity and prevalence are in line with the “atopic-march” concept of AD and subsequent type 2 inflammatory comorbidities [19]. Appropriate longitudinal studies would be required to conclusively demonstrate this atopic-march concept in the pediatric AD population in China.
Atopic type 2 inflammatory comorbidities were widely reported, with over 90% of patients reporting at least one type 2 inflammatory comorbidity; this was generally consistent across age groups (85–98%). The most frequently reported comorbidities were hay fever, asthma, seasonal allergies, and allergic rhinitis, which were reported by over 40% of patients across all age groups. These observations in the Chinese pediatric AD population align closely with previous findings from a US cross-sectional study reporting that rates of asthma and allergic rhinitis were over 30% in the pediatric AD population and that over 70% of pediatric patients with AD reported at least one type 2 inflammatory comorbidity [20]. In addition to these comorbidities, across all age categories, approximately one-third of patients with mild AD and the majority of patients with moderate AD reported at least a “very large” impact on their HRQoL. Taken collectively these observations suggest that even mild and moderate AD cases may be associated with a substantial HRQoL burden for patients.
Strengths of this study include its conservative AD definition (requiring diagnosis according to ISAAC criteria and also a report of physician confirmation of AD) and the large and nationally representative sample size in China. Unweighted and weighted data remained similar, indicating that the original sample was unbiased and representative of the population. Limitations include those inherent to similar survey-based studies, namely recall biases and self-selection biases (i.e., patients more likely to participate may inherently be more likely to have AD). More specifically, one may hypothesize that parents of children with more severe AD may have been more inclined to complete the online survey than parents of children with mild AD; additionally, socioeconomically disadvantaged families may have been less likely to have internet access and/or be computer-literate. However, as the methodology used is consistent with previous EPI-CARE reports, the data reported provide compelling evidence for comparison with similar data drawn from other countries. Lastly, it should be noted that the HRQoL findings are based on small sample sizes.



Comments (0)