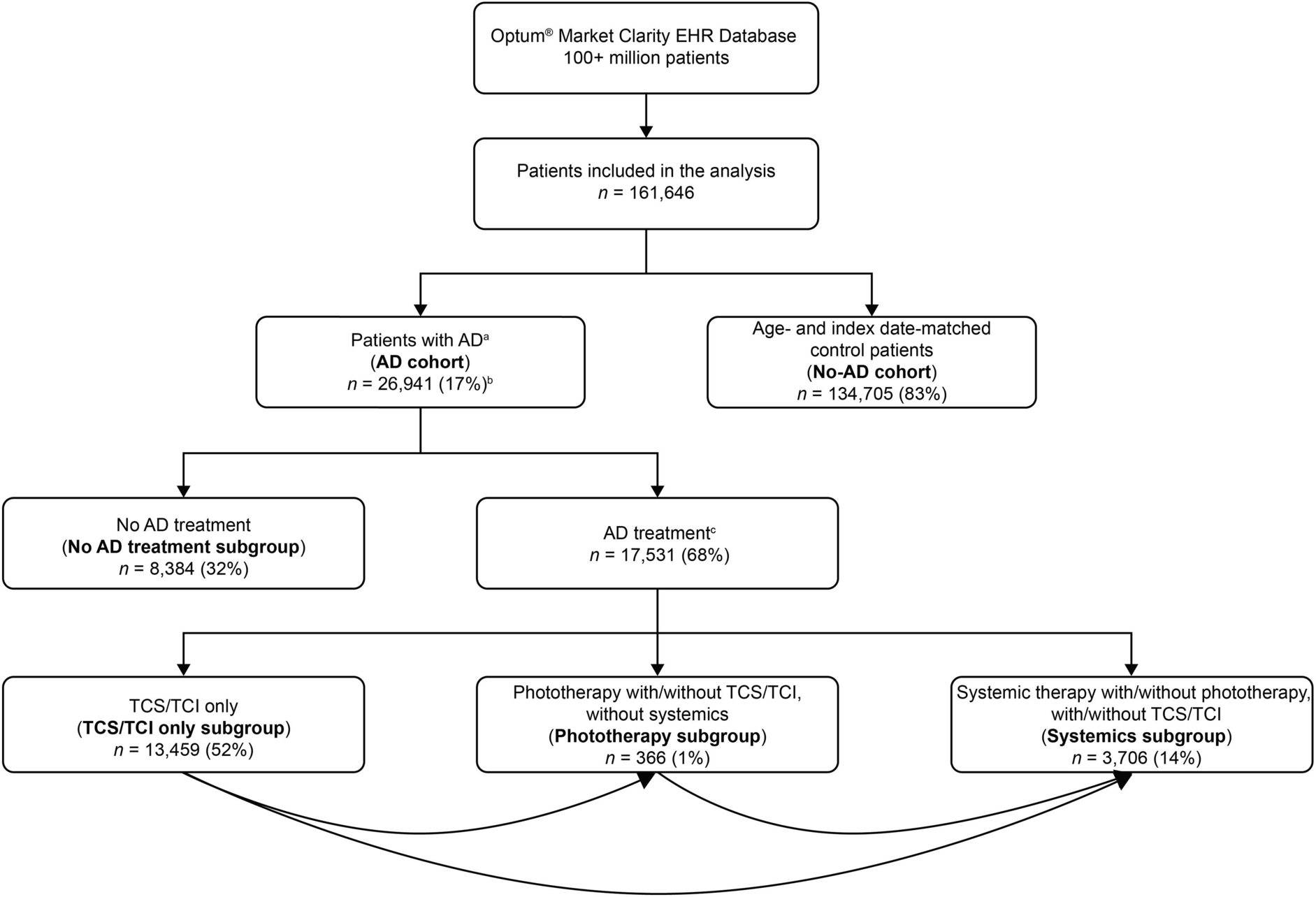
This large retrospective cohort study of EHR data from the US-based Optum® Market Clarity database examined rates of select disease events in patients with and without AD, identified based on previously reported associations and recommendations from key opinion leaders. The rates of several disease events were higher in patients with AD versus those without AD, similar to results from previous studies which identified positive associations between AD and select disease events. Crude IRs for several disease events were higher in the systemics subgroup versus the TCS/TCI only subgroup; of note, data collection occurred prior to the introduction of systemic Janus kinase (JAK) inhibitors for the treatment of AD. Our findings complement recent UK, US, and Taiwan cohort-based studies of EHR and claims data [15, 18–20, 21–25, 29, 33], which is reassuring given the inherent differences in data captured by claims (i.e., coverage decisions, resource utilization) and EHR databases (i.e., clinical decisions, practice notes, and geographic variation in coverage) [34]. Although phototherapy is not commonly prescribed for AD, we included a phototherapy subgroup in our analyses as it was recommended as a second-line treatment by relevant clinical guidelines at the time of the study [33]. A no AD treatment subgroup was included as a proxy for patients with mild AD. Surprisingly, rates of many disease events were higher in this subgroup compared with the non-AD cohort, suggesting that the no AD treatment subgroup may have included patients with uncontrolled AD of any severity level. As such, underlying comorbid conditions or prescribed treatments unrelated to AD may have contributed to higher rates of some disease events.
The risk of pneumonia, herpes simplex, and serious, and opportunistic infections was found to be higher in patients with AD versus the general UK population in previous cohort studies [11, 21], and the risk of COVID-19, conjunctivitis, and allergic conjunctivitis was found to be higher in patients with AD versus the general US population [22, 31, 32]. Although the rate of COVID-19 was assessed in the current study, COVID-19 vaccination status was not examined. In the current analysis, rates of infections were between 33% (COVID-19) and 196% (conjunctivitis) higher in the AD cohort versus the non-AD cohort, which could be attributable in part to the use of systemic therapies, which have previously been shown to increase the risk of infection and malignancies [33]. Indeed, in the current study, the rates of most infections were higher in the systemics subgroup versus the TCS/TCI only subgroup. However, as adjusted rates were also significantly greater in the TCS/TCI only subgroup versus the non-AD cohort for herpes zoster, herpes simplex, COVID-19, and conjunctivitis, the increased risk of infection in patients with AD may not be fully attributable to treatment type, and underlying disease pathogenesis may contribute to the risk of infection [36]. These findings are in line with those from previous UK-based cohort studies, which, alongside the impact of systemic therapy, highlighted the contribution of skin barrier defects and immune dysregulation to the increased risk of infection in patients with AD [11, 21].
In the current study, rates of overall malignancy (excluding NMSC), breast cancer, lymphoma, NMSC, BCC, and SCC were significantly higher in patients with AD versus patients without AD, reflecting the results of previous EHR and claims database studies conducted in the UK, Denmark, and Taiwan [19, 20, 29, 37]. In the UK, severe AD was associated with a threefold higher risk of lymphoma in adults and children with severe AD [2]. Although the pathophysiology underlying the association between AD and malignancy is unclear, immune dysfunction and chronic inflammation may contribute to the increased risk of solid organ tumors (i.e., breast cancer) in patients with AD [38, 39]. Increased skin surveillance resulting from long-term clinical monitoring may lead to greater detection of skin cancers (i.e., NMSC, BCC and SCC) in patients with AD [40]. Future studies are warranted to further elucidate the relationship between AD and malignancies.
The risk of cardiovascular events, including angina pectoris, MI, stroke, VTE, DVT, and cardiovascular death was increased in patients with AD versus demographically- and index-matched controls in Denmark, UK, Taiwan, and South Korea [13, 23,24,25]. This result is consistent with that of the present study wherein rates of all evaluated cardiovascular events were significantly higher in patients with AD versus patients without AD. As chronic systemic inflammation is common to the pathophysiology of both AD and cardiovascular disease, this factor likely contributes to the increased risk of cardiovascular events in patients with AD [41].
Similar to the current study, AD was associated with depression and anxiety in a global systematic review and meta-analysis [42], and a longitudinal study using Taiwanese claims data identified an increased risk of depression and anxiety outcomes in patients with AD versus patients without AD [43]. Furthermore, consistent with the current study, increased risks of low bone mineral density, osteopenia, osteoporosis, and related fractures in patients with AD versus patients without AD were reported in a systematic review and meta-analysis [45], which may be partly attributable to the use of systemic and topical corticosteroids [46]. Taiwan and UK population-based cohort studies have also reported that exposure to systemic corticosteroids was associated with an increased risk of fracture [34, 47].
A UK population-based cohort study reported a 4% higher risk of all-cause mortality in patients with AD versus patients without AD; however, the mortality risk was 60% higher in patients with severe AD compared with the non-AD controls, primarily due to infection and respiratory disease [47]. This is consistent with the current analysis wherein the adjusted mortality rate was 8% higher in patients with AD versus patients without AD, and 88% higher in the systemics subgroup, possibly reflecting patients with more severe disease.
Some studies have reported little to no impact of AD on the risk of select disease events, including many types of malignancies, VTE, DVT, and PE [14, 19]. This may be due to differing ICD codes used to define AD and disease events of interest. Additionally, some studies may have excluded patients with a history of comorbidities [13,14,15,16, 18,19,20,21, 23,24,25, 29, 34, 44], resulting in healthier baseline study populations.
Limitations
Previous insurance claims and EHR database studies have demonstrated poor predictive value of using ICD codes to identify AD, resulting in potential misclassification [48,49,50]. To minimize misclassification, we used ≥ 1 inpatient or ≥ 2 outpatient codes to identify patients with AD. Although previous studies have indicated that the positive predictive values of ICD codes for AD are increased when used concomitantly with codes for comorbid allergic conditions [48], this approach was not used in the current study. Misclassification of disease events was possible, and causality could not be inferred from these observational analyses. In addition, AD diagnosis prior to the study period was unknown, and the follow-up time may have been insufficient to capture rates of events with longer induction or latency periods. The use of the Optum® EHR database may have resulted in overrepresentation of patients aged ≥ 65 years (24%) and from the Midwest USA (51%). As patients with AD are more likely to visit a dermatologist and undergo close monitoring of the skin than patients without AD, these findings are subject to potential ascertainment and surveillance bias, particularly for skin cancer outcomes.
Although AD severity was not directly captured in this study, analyses were stratified by treatment subgroups, which may serve as a proxy for disease severity and is a common approach in many EHR- and claims-based studies [13,14,15,16, 18, 21, 23,24,25, 28, 33, 45, 46]. Although claims data served as proxies for AD treatment, it was not possible to verify treatment usage, and over-the-counter corticosteroid use could not be captured. In addition, these analyses did not address dosage and duration or the underlying reason for prescription, and therapies may have been prescribed off-label. Treatments may have been used for indications other than AD, potentially impacting our subgroup classification. Treatment use could itself have contributed to associations between AD and select disease events. Individual drugs within each subgroup may have different associations with each disease event. Patients with AD who received treatment for more advanced disease (e.g., systemics) may have received simultaneous treatment with phototherapy and TCS/TCI; however, associations between concurrent therapy use and disease events were not specifically examined.
Statistical adjustment controlled for known confounding variables; however, unknown confounders could not be considered. As this was an exploratory study, statistical adjustment for multiple comparisons was not made, which might have inflated the Type I error rate. Factors which may have contributed to inconsistent effect sizes and direction across categories included small sample sizes for certain disease events (e.g., tuberculosis) and treatment subgroups (e.g., phototherapy), variability in recording at the point of care, and record keeping problems inherent to all real-world data; results should be interpreted with caution. Although data were included from a large number of patients (26,941 and 134,705 in the AD cohort and non-AD cohort, respectively), repeated data binning and the rare nature of some disease events led to low event frequencies for some analyses in this study. Finally, these data may not be generalizable to the entire US population as the Optum® EHR database does not capture untreated individuals.
Conclusions
In this retrospective observational analysis of US EHR data rates of certain disease events were higher in patients with AD versus patients without AD. Rates of select disease events were generally highest in patients receiving systemic therapies and not as high in patients using only TCS/TCIs. The current study further informs the incidence of select disease events in patients with AD and may aid clinicians in predicting event risk and how AD treatments may influence these frequencies. These data may also help contextualize the safety profile of AD therapies in clinical trials.



Comments (0)