Germline GATA2 mutations are one of the most frequent constitutional defects predisposing to pediatric MDS [2]. Compared with adult MDS, GATA2-associated MDS usually presents with hypocellular BM. Second hits, such as cytogenetic changes or somatic mutations, are frequently associated with increased proliferation, resulting in changes in BM cellularity [12]. The timing for HSCT in GATA2-deficient patients without risk factors (such as cytogenetic abnormalities, severe cytopenia, severe/recurrent infections or advanced disease) is debated. Our patient, lacking such risk factors, was managed conservatively, but recent evidence highlights that somatic mutations, like ASXL1, which can be present in 20% of GATA2 patients [13, 14], can worsen outcomes [13].
Fibrosis can be detected in 10–20% of adult MDS [15] cases and up to 73% of GATA2-deficient patients [16, 17], either at initial diagnosis or during the follow-up. In MDS patients, fibrosis predicts poorer overall survival along with higher rate of leukemic transformation [15]. However, GATA2-associated MDS is now recognized as a a distinct disease entity by the International Consensus Classification (ICC) and WHO classification of myeloid neoplasms [18]. Unlike primary myelofibrosis (PMF), a myeloproliferative neoplasm characterized by stem-cell clonal myeloproliferation and driver mutations in JAK2, MPL or CALR genes [19], such mutations have not been described in large GATA2 cohorts [13, 14]. Only one case of germline GATA2 with somatic JAK2 mutation has been reported [20]. In contrast, mutations in ASXL1 and STAG2 are more commonly observed in GATA2-associated MDS, consistent with its unique pathogenesis. Our patient did not exhibit additional molecular features commonly seen in PMF, and ASXL1 mutations, while present in up to one-third of PMF patients, are less frequent in triple-negative (wild type JAK2, CALR or MPL) individuals [19].
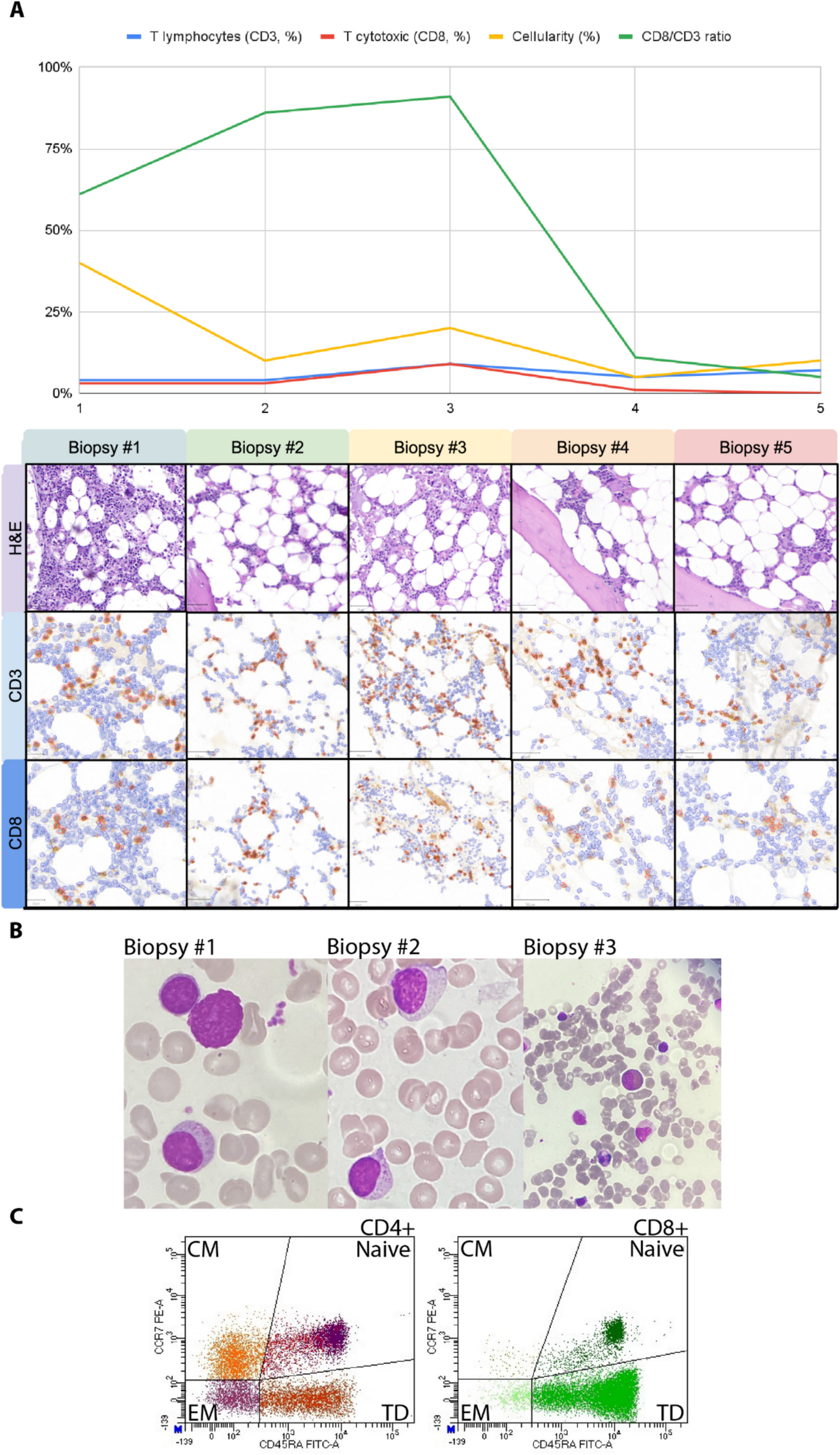
How fibrosis in GATA2-deficient patients relates to immune dysfunction remains unclear. Although in PMF percentages of CD4, CD8 and their subsets have been shown to be similar either in PB or BM [21], decreasing CD8+ T-cell counts in BM are associated with progression from low-risk to high-risk MDS [3]. Here we describe that inverted PB CD4:CD8 ratio, T-cell counts and subsets remained stable during follow-up with expansion of CD4 and CD8 TEMRA and reduction of BM CD8+. Thus, in GATA2 deficiency, BM CD8+ seems to follow the MDS progression rather than PMF evolution, possibly reflecting immune surveillance escape and impaired anti-tumor activity.
T-cell exhaustion and functional impairment of cytotoxic T-cell, inverted CD4:CD8 ratio and restricted and activated T-cell repertoire have been related to tumor microenvironment, age-related changes, chronic viral infections and have been described either in PMF [21] and MDS [3]. Abnormal patterns of T-cell gene rearrangements were reported in the BM of GATA2 individuals [16, 17]. PB or BM flow cytometry showed inverted CD4:CD8 ratio in GATA2 patients [4, 16]. Ruiz-Garcia et al. [4] reported an association between increased PB CD8+ TEMRA and a more severe phenotype in GATA2 patients. However, these findings require further validation due to several limitations. First, increased TEMRA percentages were observed in only two out of four patients. Second, the analysis relied solely on percentages without providing absolute cell counts, which limits interpretability. Finally, these patients, in contrast to our case, had a long history of severe and recurrent infections, which could independently influence CD8+ TEMRA dynamics. Therefore, while these observations are intriguing, additional studies with larger cohorts and comprehensive immunophenotyping are needed to confirm these findings. Dysfunctional CD8+ anti-tumor activity and immune surveillance escape have been linked to the CD8+ exhausted phenotype and impaired metabolic activity. Experimental approaches, such as inhibitory receptors blockade or mitochondrial transfer, have been shown to effectively reverse the CD8+ exhausted phenotype and ultimately enhance the CD8 anti-tumor activity [22, 23]. While these therapies are not intended to address the BM failure or multilineage cytopenia that necessitate HSCT in GATA2 deficiency, the exhausted CD8+ phenotype and the mitochondrial defect observed in GATA2-deficient CD34 + cells [24], suggest that similar mechanism may contribute to immune dysfunction. A deeper understanding of the alterations in GATA2-deficient CD8+ cells could lead to future strategies to restore immune surveillance, complementing standard treatments like HSCT.
The limitations of this study include its retrospective nature and reliance on a single patient, highlighting the need for confirmation in larger, prospective cohorts. Additionally, PB samples were not available, preventing a comparative assessment of the percentage of LGL between the BM and PB. Lastly, LGL phenotyping was not performed, restricting the ability to precisely determine whether the LGL were of T or NK lineage.
Our case shows that, even in young adults and in the absence of chronic viral infections, GATA2 BM microenvironment may recapitulate MDS BM abnormalities and be associated with progressive triple-negative marrow fibrosis. Monitoring of BM CD8+ could be of use in GATA2 deficiency. Further studies regarding BM T-cell phenotype, gene, protein, and metabolic profiles will shed a light into GATA2 BM microenvironment and MDS evolution.



Comments (0)