
Remember me
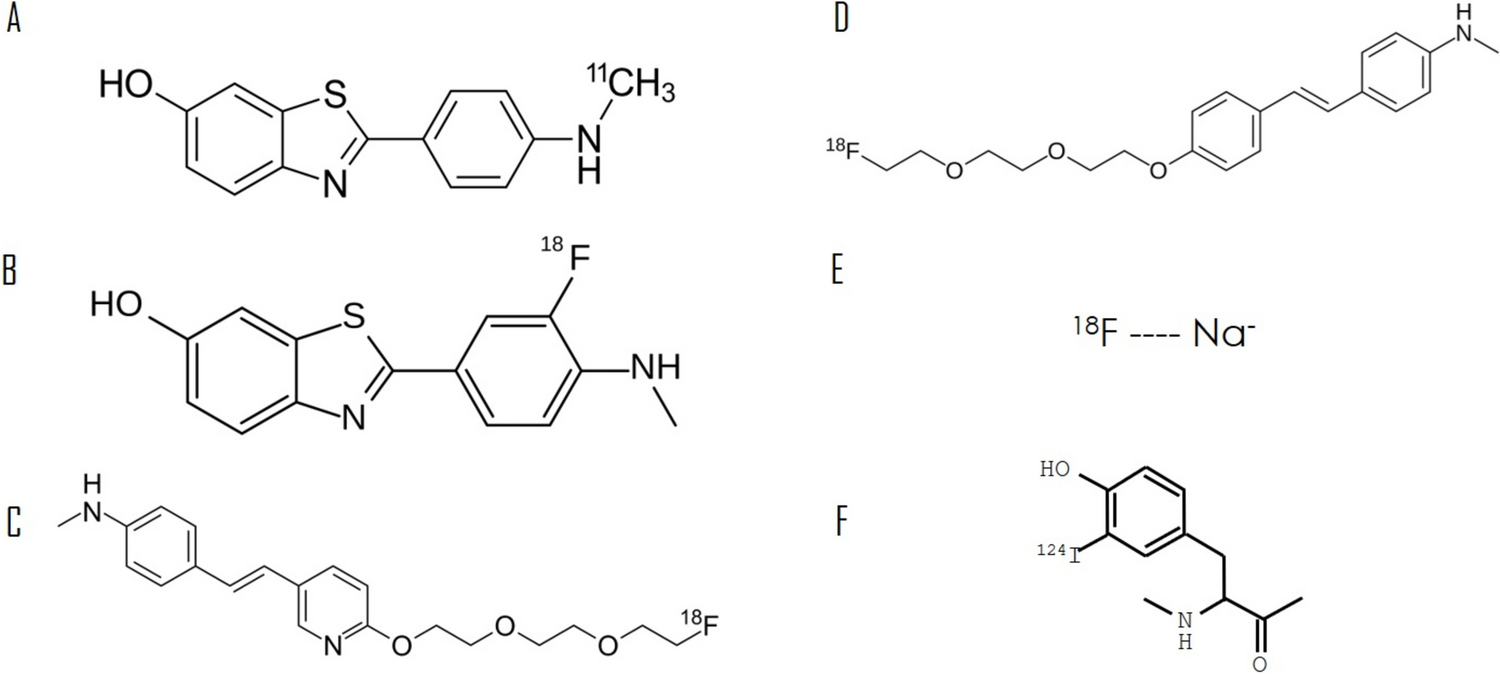

[11C]PiB is a radioactive analog of thioflavin T (Fig. 1). Given the short half-life of 20.4 min, the primary limitation of [11C]PiB PET is the requirement for an on-site cyclotron to produce the tracer [13]. This tracer has not been approved by the FDA.
Fig. 1
Molecular structures of various amyloid radiotracers. A [11C]Pittsburgh compound B by Ed (Edgar181)—own work, public domain, https://commons.wikimedia.org/w/index.php?curid=65798106. B [18F]Flutemetamol by Anypodetos—own work, CC0, https://commons.wikimedia.org/w/index.php?curid=35531313. C [18F]Florbetapir by Ed (Edgar181)—own work, public domain, https://commons.wikimedia.org/w/index.php?curid=21718327. D [18F]Florbetaben by Ed (Edgar181)—own work, public domain, https://commons.wikimedia.org/w/index.php?curid=31776306. E 18F-sodium fluoride. F [124I]Evuzamitide: the alpha helix with charged lysine side chains
DiagnosisIt enables detection and quantification of β-amyloid deposits in AD [14, 15]. A pioneering study in 2013 demonstrated that [11C]PiB imaging could also detect CA. The authors observed myocardial [11C]PiB uptake in 10 patients with either AL- or ATTR-CA, with no uptake in 5 healthy controls [16]. Subsequent case–control studies have confirmed the specificity of [11C]PiB uptake in CA. For instance, a study involving 22 patients with monoclonal gammopathy showed [11C]PiB uptake in 13 out of 15 patients with biopsy-confirmed CA, and no uptake in patients without CA [17]. Another study reported significantly greater myocardial [11C]PiB uptake in patients with AL-CA (n = 41) compared to 14 healthy subjects [17]. Further research involving 36 patients with AL-CA, 21 with ATTR-CA, and 15 with non-amyloid left ventricular (LV) hypertrophy or healthy volunteers revealed the diagnostic accuracy of [11C]PiB uptake visual inspection to be 100% in differentiating CA patients with increased wall thickness from controls. This study also suggested that [11C]PiB could detect early-stage CA, as some patients with amyloidosis but no known cardiac involvement, defined as LV wall thickness > 12 mm in the absence of other cause of hypertrophy, exhibited [11C]PiB [18]. Additionally, [11C]PiB uptake was significantly higher in AL-CA than in ATTR-CA: at 10 to 20 min after [11C]PiB injection, AL patients had the highest standardized uptake value (SUV) (2.61) and retention index (RI) (0.086 min−1), followed by ATTR patients (SUV 1.64, RI 0.045 min−1) and controls [18].
In another study with 47 patients (17 AL, 22 ATTRv, 8 ATTRwt), a combined approach of [11C]PiB PET and [99mTc]PYP scintigraphy allowed accurate differentiation between AL- and ATTR-CA. All patients with AL-CA exhibited positive [11C]PiB and negative [99mTc]Tc-PYP uptake (“PiB pattern”), and all patients with ATTRwt-CA showed the opposite pattern (“PYP pattern”) [19, 20]. Myocardial [11C]PiB uptake also correlated with the amount of amyloid deposits on histology, evaluated as the percentage of amyloid-positive area in amyloid P immunohistochemistry slides [17].
Furthermore, native T1 mapping values positively correlated with target-to-background ratio (TBR) max values (considering a cut-off of 1.09; sensitivity 92.3% and specificity 100%) in CA and non-CA patients who underwent cardiac [11C]PiB PET/MRI [21].
Risk predictionMyocardial [11C]PiB uptake independently predicted clinical outcomes in AL-CA, with patients having the highest PiB uptake experiencing the shortest event-free survival [17]. In a prospective study on 58 patients with AL-CA, myocardial [11C]PiB uptake emerged as a strong independent predictor of 1-year overall mortality and refined risk prediction beyond the traditional AL-CA staging system, based on commonly used serum biomarkers, such as troponin I, N-terminal pro-B-type natriuretic peptide, and the difference between free light chains [22]. Although some other reports have suggested a potential role for [11C]PiB PET in risk stratification [23], larger-scale studies are necessary to confirm these findings.
MonitoringIn a case report by Fujioka et al., [11C]PiB PET/CT was employed to monitor a patient on tafamidis and demonstrated a reduction in amyloid deposition after almost 1 year of treatment [24]. Although the tracer uptake correlates with the degree of amyloid deposition, there are no studies on AL-CA exploring the potential application of [11C]PiB PET scans in determining whether amyloid clearance is correlated with clinical response [25].
18F-flutemetamolChemical structure, half-life, and FDA approval[18F]Flutemetamol is structurally similar to [11C]PiB but features a 3’ [18F] fluorine substitution [26]. [18F]Flutemetamol has a half-life of 110 min, allowing its distribution to PET centers without on-site cyclotrons [27]. It is the second 18F-labeled PET radiopharmaceutical approved by the Food and Drug Administration (FDA) for in vivo detection of amyloid deposits in 2013 [28]. The first report of myocardial retention of [18F]Flutemetamol in CA (specifically in AL-CA) was published in 2014 [29].
DiagnosisA 2019 pilot study assessing the diagnostic properties of [18F]Flutemetamol PET in CA included 9 CA patients (8 with ATTR and 1 with AL) and 3 controls without CA. The study observed [18F]Flutemetamol uptake in 8 of the 9 CA patients and none of the controls during a 30-min list-mode acquisition, a data collection technique in which detector counts are stored sequentially as scan time progresses. The median TBR was significantly higher in CA patients than controls, with the single AL-CA patient showing a higher TBR than those with ATTR-CA (1.46, IQR 1.32–2.06 versus 1.06, IQR 0.72–1.1, p = 0.033) [30] (Fig. 2). In 2020, a study involving 21 patients with V30M ATTRv-CA and 6 controls (5 AD patients and one healthy individual) evaluated 18F-flutemetamol uptake over a 60-min dynamic PET acquisition. This study found 88% sensitivity and 100% specificity in identifying ATTRv-CA patients at 30- or 60-min static image acquisitions. The authors proposed a SUV cut-off of 1.46 for the intraventricular septum at 30 min as a diagnostic cut-off [31]. Another retrospective study investigated [18F]Flutemetamol uptake in 12 CA patients (7 ATTRwt, 3 ATTRv, 2 AL) and 5 with non-amyloid heart failure, with acquisition times set at 60 to 90 min post-injection. The study found no significant difference in quantitative tracer uptake between the two groups, and increased uptake was observed in only 2 of the 12 amyloidosis patients, suggesting that late acquisition is not sensitive for detecting cardiac amyloid deposits [32].
Fig. 2
[18F]Flutemetamol imaging in subject with cardiac amyloidosis. a Showing high radiotracer uptake in the left and in the right myocardium, versus a representative control. b with no significant uptake in the myocardium, including in columns from the left to the right: maximum intensity projections (MIP), fused positron emission tomography (PET)/computed tomography (CT), CT, and PET. Reprinted with permission from [30]
Risk prediction and monitoringFurther research is necessary to establish the specific acquisition protocol and the diagnostic accuracy of [18F]Flutemetamol in CA, as well as to explore the potential of its use in prognostic stratification and the assessment of therapeutic response, as in an ongoing trial (NCT05374564) conducted on 12 patients comparing the disease burden at 0 and 6 months of treatment with tafamidis.
Cyano-flutemetamol is an [18F]Flutemetamol analog with the addition of a cyano group, allowing to assess tracer binding to amyloid on histology. It binds amyloid deposits with a good agreement with Congo red and [11C]PiB, and a greater affinity for ATTR than AL amyloid. In a post-mortem histofluorescence analysis, the density of cyano-flutemetamol displayed a robust correlation with LV septal and posterior wall thickness, and LV mass [25].
[18F]FlorbetapirChemical structure, half-life, and FDA approvalSimilar to the other [18F] radiolabeled tracers, the longer half-life (110 min) of this aromatic ether represents a huge advantage respect to [11C]PiB [33]. In 2012, the FDA approved the first β-amyloid imaging PET probe for the in vivo detection of amyloid deposits in AD, as it has a high affinity for β-amyloid [34, 35].
DiagnosisThe possibility to discriminate CA from healthy controls emerged from an autoradiography study performed on autopsy samples from AL, ATTR-CA, and controls [36] and in a pilot study conducted on 9 CA patients (5 AL, 4 ATTR) and 5 controls (3 healthy subjects and 2 with non-ischemic heart failure) [37]. Using a 60-min scan duration, the LV RI, TBR, myocardial SUV, and myocardial-to-liver SUV were all higher in CA patients compared to controls. A trend towards a higher RI was observed in AL-CA patients compared to those with ATTR-CA [37]. Osborne et al. found that the uptake time before the acquisition, the length of the acquisition, and the window/level setting all significantly impacted the capability to detect and identify the differences between controls and disease populations; so, they developed a 20-min list-mode protocol with acquisition windows at 0–5, 10–15, or 15–20 min that can be easily reproduced by any trained imaging specialist at any PET center [38].
Risk predictionLV amyloid burden measured by [18F]Florbetapir PET/CT is a powerful predictor of cardiovascular events in AL amyloidosis, according to the 2012 Mayo stage, as the link between amyloid burden and cardiovascular events was mainly mediated by NT-proBNP, a component of Mayo stage [39]. Interestingly, [18F]Florbetapir PET/CT could detect early right ventricular (RV) amyloid in systemic AL amyloidosis before the occurrence of changes in RV structure and function, and predicts cardiovascular events [40].
MonitoringA small study of 15 patients assessed the possible use of [18F]Florbetapir PET to monitor AL-CA progression before and after chemotherapy. The study observed greater cardiac uptake in chemotherapy-naïve patients compared to those already undergoing chemotherapy (RI 0.21 vs. 0.14 min−1), and in patients without at least a partial hematological response (RI index 0.2 vs. 0.14 min−1). To date, no correlations between changes in cardiac uptake, cardiac biomarkers, or serum free light-chains were noted, but larger studies are needed to explore the potential role of this tracer [41].
[18F]FlorbetabenChemical structure, half-life, and FDA approval[18F]Florbetaben, an 18F-labeled stilbene derivative with a high affinity for brain β-amyloid, shares structural features with [11C]PiB, and has a half-life of 110 min. It was approved by FDA in 2014 [42].
DiagnosisIn a pilot study, 10 CA patients (5 ATTR and 5 AL) and 4 hypertensive heart disease controls were examined. All patients with AL- or ATTRwt-CA had histological disease confirmation. LV SUV was measured on static images taken between 5 and 10 min after injection. The study reported increased myocardial uptake in all CA patients, with significantly higher TBR and SUV values, in particular for AL-CA patients. This study also suggested a correlation between tracer retention and left ventricular ejection fraction on echocardiography [43]. The diagnostic value of [18F]Florbetaben PET was confirmed in a study assessing 9 patients with known or suspected CA (7 with biopsy-proven systemic AL amyloidosis, 5 with known cardiac involvement). The authors reported an intense myocardial uptake in patients with biopsy-confirmed CA, whereas those without CA showed low myocardial uptake [44]. A 2019 study by Kircher et al. with 22 patients (12 AL, 5 ATTR, 2 AA) suggested a role for [18F]Florbetaben PET in distinguishing between AL- and ATTR-CA [45]. PET images were dynamically acquired for 30 min post-injection, with static reconstructions between 10 and 30 min for visual evaluation. This study introduced the idea of discriminating between AL- and ATTR-CA through semi-quantitative evaluation of radiotracer uptake, evaluated at a later time interval than the previous pilot study [43]. Indeed, in 30 min of total imaging duration, myocardial tracer retention (MTR) values were significantly higher in AL-CA patients (median MTR of 66 with a range of 38–111) than those with ATTR-CA (median MTR of 42 with a range of 38–45, p < 0.01) and controls (median MTR of 27, under the detected cut-off of 36 to distinguish CA from non-CA), and correlated well with echocardiographic parameters, LV wall thickness (r = 0.46, p < 0.05) and apical sparing of the longitudinal strain pattern (r = 0.52, p < 0.02) [45].
In 2020, Genovesi et al. conducted a study on 40 CA patients (20 AL and 20 ATTR) and 20 with LV hypertrophy. They performed dynamic PET scans from tracer injection for 60 min and delayed static scans at approximately 110 min. This delayed acquisition allowed to reliably distinguish AL-CA (early SUV 5.55; delayed SUV 3.50) from ATTR-CA (early SUV 2.55; delayed SUV 1.25) or LV hypertrophy (early SUV 3.50; delayed SUV 1.40) (Fig. 3) [46].
Fig. 3
[18F]Florbetaben positron emission tomography for the differential diagnosis between cardiac amyloid subtypes and mimicking conditions. (Upper panel) Time–activity curves for myocardial uptake in cardiac positron emission tomography using [18F]Florbetaben are shown for patients with immunoglobulin light-chain amyloidosis (AL) (blue), transthyretin amyloidosis (ATTR) (red), and non-cardiac amyloidosis (non-CA) (gray). Shaded areas indicate the 95% confidence interval for each curve. (Lower panel) Early-phase (5–15 min), intermediate-phase (30–40 min), and late-phase (50–60 min) [18F]-florbetaben PET scans are displayed for patients with AL and ATTR cardiac amyloidosis (CA) and non-CA. SUVmean represents the mean standardized uptake value. Reprinted with permission from [46]
Then, Santarelli et al. evaluated 21 CA patients (11 AL and 10 ATTR) and 15 controls with non-amyloidotic cardiomyopathy. This study confirmed that [18F]Florbetaben affinity for amyloid substance is greater in AL-CA [47]. The same authors then investigated deep-learning tools to characterize CA deposits by evaluating static images acquired early (15 min) after radiopharmaceutical injection. The study included 47 subjects (13 ATTR-CA, 15 AL-CA, 19 non-amyloidotic cardiomyopathy), finding high accuracy, sensitivity, and specificity in distinguishing CA from non-CA and AL- from ATTR-CA [48]. Further studies on larger populations are needed to confirm the minimum time required from tracer injection to acquisition and to validate the utility of deep-learning techniques in assisting human interpretation.
Risk prediction and monitoringThe prognostic significance of the tracer remains to be explored. Vergaro et al. recently explored the prognostic significance of [18F]Florbetaben uptake in 40 patients with AL-CA: a late LV total amyloid burden ≥ 273 cm3 and late right ventricle total amyloid burden ≥ 135 cm3 predicted 18 and 24-month all-cause mortality independently from Mayo stage [49]. The ongoing phase 3 trials PETAL (NCT06048601) and CARdiag (NCT05184088) are investigating the diagnostic performance for visualizing and quantifying amyloid in patients with suspected AL-CA.
18F-sodium fluorideChemical structure, half-life, and FDA approvalBecause of the better properties of 99mTc-labeled molecules such as half-life major than the one of [18F]-radiolabeled tracers, they replaced one of the earliest radiopharmaceuticals, [18F]-NaF, for imaging applications in the 1970s. Despite approval in 1972 for use in bone scans, the ionic compound comprised of a single sodium atom bound to a positron-emitting isotope of fluorine [18F]-NaF was withdrawn in 1975. In the 1990s, advancements in PET scanners enabled better imaging, leading to its return in 1993 and FDA approval in 2000 [50].
DiagnosisThe diagnostic value of [18F]-NaF PET has been explored based on the notion that different amyloid proteins impact calcium homeostasis. In 2016, Van Der Gucht for the first time demonstrated in two patients that [18F]-NaF PET/CT could differentiate ATTR-CA from AL-CA with a faster kinetics and then imaging time than 99mTc-labeled diphosphonates: [18F]-NaF images showed a diffuse myocardial uptake in the ATTR-CA patient in the early phase, more than in the delayed phase, reflecting a faster wash-out; the AL-CA patient had no myocardial uptake at both acquisition times, indicating a different affinity for the tracer [51]. In recent studies, including two series each comprising 7 CA patients (one with 5 ATTR-CA + 2 AL-CA, the other 4 ATTR-CA + 3 AL-CA), the authors confirmed higher myocardial [18F]-NaF uptake in ATTR-CA compared to AL-CA [52, 53]. The first series utilized PET/CT 1 h post-injection, revealing a 58% higher mean SUV over the entire myocardium in ATTR-CA than in AL-CA patients, with variations in uptake intensity across myocardial segments [52]. The second series employed PET/MRI with a dynamic acquisition over 90 min starting 5 min post-injection, finding myocardial TBR values 48% higher in ATTR CA than in AL CA patients, exhibiting a patchy pattern of uptake [53]. In a larger cohort with suspected CA, [18F]-NaF PET/MRI showed its capability to distinguish ATTR from AL amyloidosis and non-amyloid patients, particularly when myocardium to blood pool ratio semi-quantification was used, as visual interpretation displayed lower contrast [54].
A study found a significantly higher TBR in ATTR-CA (n = 7) (0.98 ± 0.09) as compared to AL-CA (0.85 ± 0.08; p = 0.026) and controls (0.82 ± 0.07; p = 0.020), suggesting that a TBR cut-off of 0.89 could discriminate the 2 types of CA [55]. In a study of quantitative 18F-fluoride PET/magnetic resonance imaging (MRI), TBR was significantly higher in patients with ATTR-CA (n = 10) (1.13 ± 0.16) than healthy controls (0.84 ± 0.11, p = 0.0006) and other similar phenotypes, such as patients with aortic stenosis (0.73 ± 0.12; p < 0.0001) or AL-CA (0.95 ± 0.08; p = 0.01). Moreover, linking TBR PET-findings with late gadolinium enhancement on cardiac MRI could get higher specificity and sensitivity to distinguish ATTR-CA and AL-CA [56] (Fig. 4). Despite these promising findings, [18F]-NaF PET/CT remains inferior in terms of sensitivity with a value of 0.25 (95% CI 0.089 to 0.53) compared to [99mTc]Tc-PYP single-photon emission computerized tomography (SPECT) (100%, p = 0.016) for the diagnosis of ATTR-CA [57].
Fig. 4
Patterns of [18F]-fluoride uptake between cohorts. Columns represent each cohort and rows imaging modality in the short axis view. Panel A shows a delayed enhanced image of a control subject with normal myocardial mass and no late godolidium enhancement (LGE). The corresponding fused positron emission tomography/magnetic resonance (PET/MR) image (E) shows uptake only in the blood pool. Panel B is a patient with aortic stenosis and elevated left ventricular mass. Note the absence of myocardial.18F-fluoride uptake on panel F and similar to the healthy control, uptake is greater in the blood pool than myocardium. Panel C shows a patient with light-chain (AL) amyloid displaying the characteristic myocardial nulling difficulties with LGE found in cardiac amyloidosis. Panel G shows patchy lateral wall uptake greater than the blood pool. Panel D shows similar LGE findings, but this time in transthyretin (ATTR) amyloid. Note the striking and extensive biventricular uptake in panel H, much greater than the blood pool and what was seen in AL. Target-to-background ratio (TBR). Reprinted with permission from [56]
Risk prediction and monitoringTo date, no data is available on the use of tracers for prognosis definition and therapy response monitoring.
[124I]EvuzamitideChemical structure, half-life, and FDA approvalEvuzamitide, also known as p5 + 14, is a pan-amyloid-reactive peptide, binding all forms of amyloid, included AL kappa, AL lambda, ATTRv, leukocyte chemotactic factor-2, apolipoprotein-A2c, serum amyloid A, and islet amyloid polypeptide, derived from various anatomic sites, overcoming the problem of the etiological heterogeneity of this systemic disease [58]. In August 2024, the FDA granted its breakthrough therapy designation to the PET [124I]Evuzamitide for imaging in patients with suspected or known CA. The completion of the phase 3 REVEAL study (NCT06788535) evaluating the efficacy and safety of [I-124]Evuzamitide is estimated for the end of 2025. This peptide labeled with iodine-124 is a cyclotron-produced radionuclide with a 4.2-day half-life.
DiagnosisA single-site, open-label first-in-human phase 1/2 study (NCT03678259) substantiates the general safety and effectiveness of [124I]Evuzamitide—in identifying cardiac and systemic amyloid deposits with high sensitivity (93.6%) in 50 patients with systemic amyloidosis, 2 asymptomatic ATTRv carriers, and 5 healthy volunteers [59]. As patients involved in this study presented different types of systemic amyloidosis, [124I]Evuzamitide PET showed different patterns of cardiac uptake: although right ventricular and atrial walls were also observed in certain patients with AL, ATTR, lysozyme, and apolipoprotein-A1 amyloidosis, the LV, particularly the interventricular septum and posterior wall, was the primary site of myocardial uptake of [124I]Evuzamitide; then, only trace blood pool activity was observed in the ventricular lumen in patients with leukocyte chemotactic factor-2, gelsolin, and healthy people, suggesting no amyloid deposits in the myocardium [58] (Fig. 5). A pilot study including 46 participants (12 AL-CA, 12-ATTRwt, 2 ATTRv, and 20 controls without CA) compared [18F]Florbetapir and [124I]Evuzamitide, finding a comparable discrimination performance for the two tracers in AL-CA, and a preferable application of [124I]Evuzamitide in ATTR-CA. Moreover, this study revealed the correlation between the radiotracer uptake and morphologic and functional cardiac parameters measured with echocardiogram and MRI, such as interventricular septum thickness (Spearman’s ρ = 0.78), LV global longitudinal strain (ρ = 0.54), LV mass index (ρ = 0.82), and extracellular volume (
Comments (0)