Medical therapy
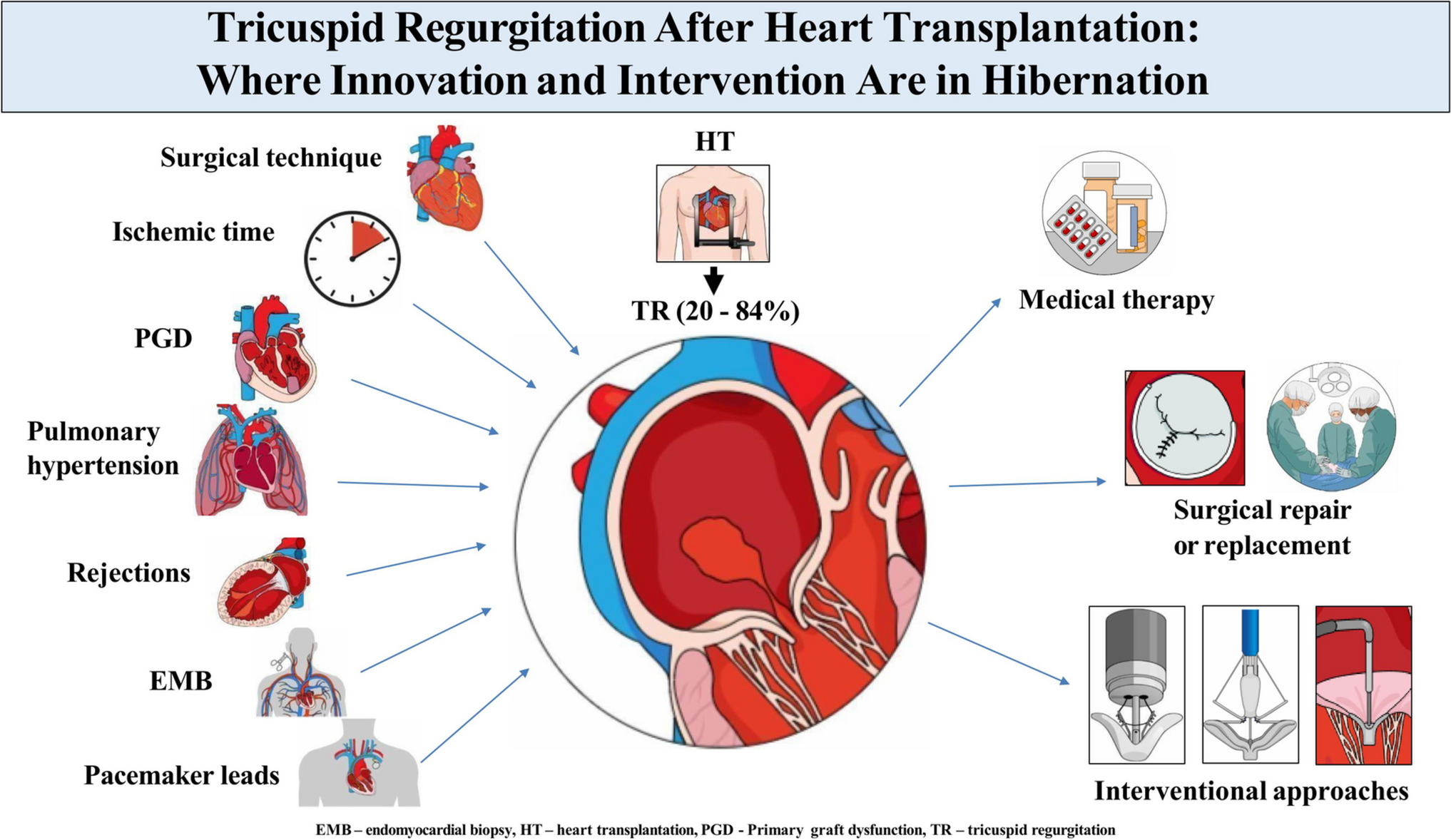
The mainstay of therapy for symptomatic severe TR after HT is medical management. This approach focuses on optimizing patient medication, managing volume overload with diuretics, and addressing any contributing factors, such as arrhythmias or pulmonary hypertension.
Interventional or surgical treatment is generally reserved for a minority of patients in whom TR results in refractory symptoms despite optimal medical therapy. However, patient selection for these interventions remains critical, as the clinical benefit must outweigh the procedural risks in this unique patient population.
Surgical techniquesTricuspid annuloplasty (TA)
The management of TR after HT involves several surgical options aimed at reducing its severity. Techniques such as Carpentier’s ring annuloplasty, the De Vega technique, and valve replacement are commonly utilized [4, 27, 28].
The Carpentier technique involves the systematic repair of tricuspid valve incompetence by assessment of the valve for any organic lesions, such as leaflet thickening, commissural fusion, and annular deformation using obturators. If the annulus is dilated or deformed, the technique employs a remodeling approach using prosthetic rings, which are shaped and sized based on measurements of the anterior leaflet. This method selectively reduces the annulus at points of excessive dilation, particularly the commissures, while maintaining the valve’s shape to avoid stenosis [27].
The De Vega annuloplasty technique is a surgical procedure designed to treat functional TR by reducing and stabilizing the size of the tricuspid annulus. The procedure involves the placement of a double continuous suture along the dilated portions of the tricuspid annulus, mainly focusing on the anterior and posterior segments, which are prone to dilation. The sutures are carefully placed to avoid the septal portion of the annulus, thereby protecting the conduction system. This technique is favored due to its simplicity, effectiveness, and ability to be performed by less experienced surgeons, with low rates of reoperation for recurrent TR [28].
Both the Carpentier and De Vega annuloplasty techniques have been utilized as treatment options for TR in HT recipients. TA performed during the HT process has demonstrated efficacy in mitigating early postoperative TR. For example, a study comparing 25 patients who received donor heart TA with either the De Vega or Carpentier’s ring techniques to a cohort of 25 patients who did not undergo TA found that preemptive TA significantly reduced postoperative TR, as evidenced by lower TR scores on early echocardiograms [4]. However, TA in HT is also linked to a higher occurrence of conduction abnormalities, such as right bundle branch block (37% vs. 9% in non-TA patients) and complete heart block, resulting in more frequent pacemaker implantations. While TA effectively prevents severe TR, it does not offer significant long-term hemodynamic benefits [29]. The studies by Jeevanandam et al. address the debate over the timing and impact of surgical tricuspid valve repair in HT. Their 2004 study demonstrated that prophylactic donor TA improved renal function but did not significantly enhance survival rates [30]. In a follow-up 2006 study, the prophylactic approach was still beneficial in preventing severe TR, but it did not lead to substantial long-term improvements in overall survival or hemodynamics [31]. These findings suggest that while donor TA may have some short-term advantages, its long-term benefits in terms of survival and cardiac function remain uncertain. Prophylactic TA during HT can increase the risk of right heart failure, particularly when pulmonary arterial hypertension is present. This is because, without the natural “pressure relief” function of the TR, the RV may struggle to manage the increased pressure. Conversely, moderate to severe TR, coupled with pulmonary hypertension, can exacerbate RV dysfunction by leading to volume overload and eventual right heart failure [25, 32, 33].
Surgical tricuspid valve replacement (sTVR)
sTVR has proven to be an effective approach for managing severe TR in HT recipients when medical therapy alone is inadequate, although based on evidence from case reports and small, single-center studies [34, 35]. In a study of 163 HT patients, nine individuals received TVR due to significant TR that developed an average of 5 years after the transplant. The treatment significantly reduced TR severity in all cases, leading to substantial clinical benefits, including an average 24% reduction in serum creatinine and a 47% decrease in total bilirubin. Patients also reported improved symptoms and reduced diuretic use [35]. These findings highlight TVR as a promising treatment for severe TR in post-transplant patients, although careful patient selection is crucial to minimize risks and optimize outcomes. In the study by Raghavan et al., the types of valves used for sTVR are not mentioned [35]. In contrast, the case report by Votapka et al. specifies the use of a Hancock porcine valve for sTVR [34]. Compared to biological valves, mechanical valves for TVR in HT recipients have several drawbacks, including the need for anticoagulation and the inability to perform EMBs.
Interventional approachesTranscatheter tricuspid valve repair (tTVr)
The complexity of the tricuspid valve anatomy, including the large annulus, dense chordae, and the challenging geometry of the valve in HT recipients, poses significant technical difficulties in the development and application of transcatheter therapies for TR. So far, the interventional treatment of TR in HT recipients is a field, with most available evidence derived from case reports and small case series. One of the earliest transcatheter techniques employed for managing TR was edge-to-edge repair using the MitraClip device. This approach was employed successfully until the introduction of dedicated transcatheter techniques specifically designed for TR.
Successful TR repair with the MitraClip was initially described in a 20-year post-HT patient, resulting in significant symptomatic improvement and TR reduction [36]. A subsequent report documented successful percutaneous treatment of severe TR in two elderly HT patients. Both patients had developed severe TR due to multiple EMBs that caused leaflet flail, and they were at high risk for sTVR. The tTVr procedure led to a significant reduction in TR, with normalization of right ventricular size and function. Both patients had excellent clinical outcomes, remaining stable and independent during a 2-year follow-up period [37].
In a case series of seven HT recipients (median age 53, predominantly female), transcatheter tricuspid valve edge-to-edge repair (T-TEER) was performed using the TriClip device. The procedure, which involved implanting 2–3 clips in a tricuspid position, was technically successful in six of the seven patients. In one patient, however, due to a single leaflet device attachment, a second clip was used to stabilize the detached leaflet. The intervention resulted in significant TR reduction and right ventricular remodeling at follow-up. Most patients were discharged within 2–4 days without in-hospital adverse events. During a median follow-up of 13 months, one patient died from non-cardiac causes (perforated diverticulitis with burst abdomen, compounded by a suspected acute rejection and right heart failure, despite the near-optimal reduction of TR), while the remaining six experienced improved NYHA functional class, suggesting that T-TEER is a promising, minimally invasive alternative for managing TR in this high-risk population [38]. A TriClip device was also used for percutaneous tricuspid repair in a 67-year-old HT patient with severe TR, resulting in a successful reduction of the regurgitation [39]. Another device is the PASCAL Ace system, which has been used successfully in two HT patients in an initial case series [40].
Transcatheter tricuspid valve replacement (tTVR)
Currently, there are no reports on the use of tTVR systems, such as EVOQUE, in HT recipients. However, in the TRISCEND trial, elderly patients with multiple comorbidities and at least moderate TR demonstrated sustained TR reduction and significant improvements in cardiac output, along with high survival rates and reduced hospitalizations after tTVR [41]. HT patient recipients are often high-risk surgical candidates due to factors such as immunosuppressive therapy, prior surgeries, and various comorbidities, which make them less suitable for traditional surgical repair or replacement. While transcatheter interventions show promising early results, they remain relatively novel in HT recipients. Consequently, larger randomized studies are needed to further evaluate their long-term efficacy and safety in this special patient population.


Comments (0)