
Remember me

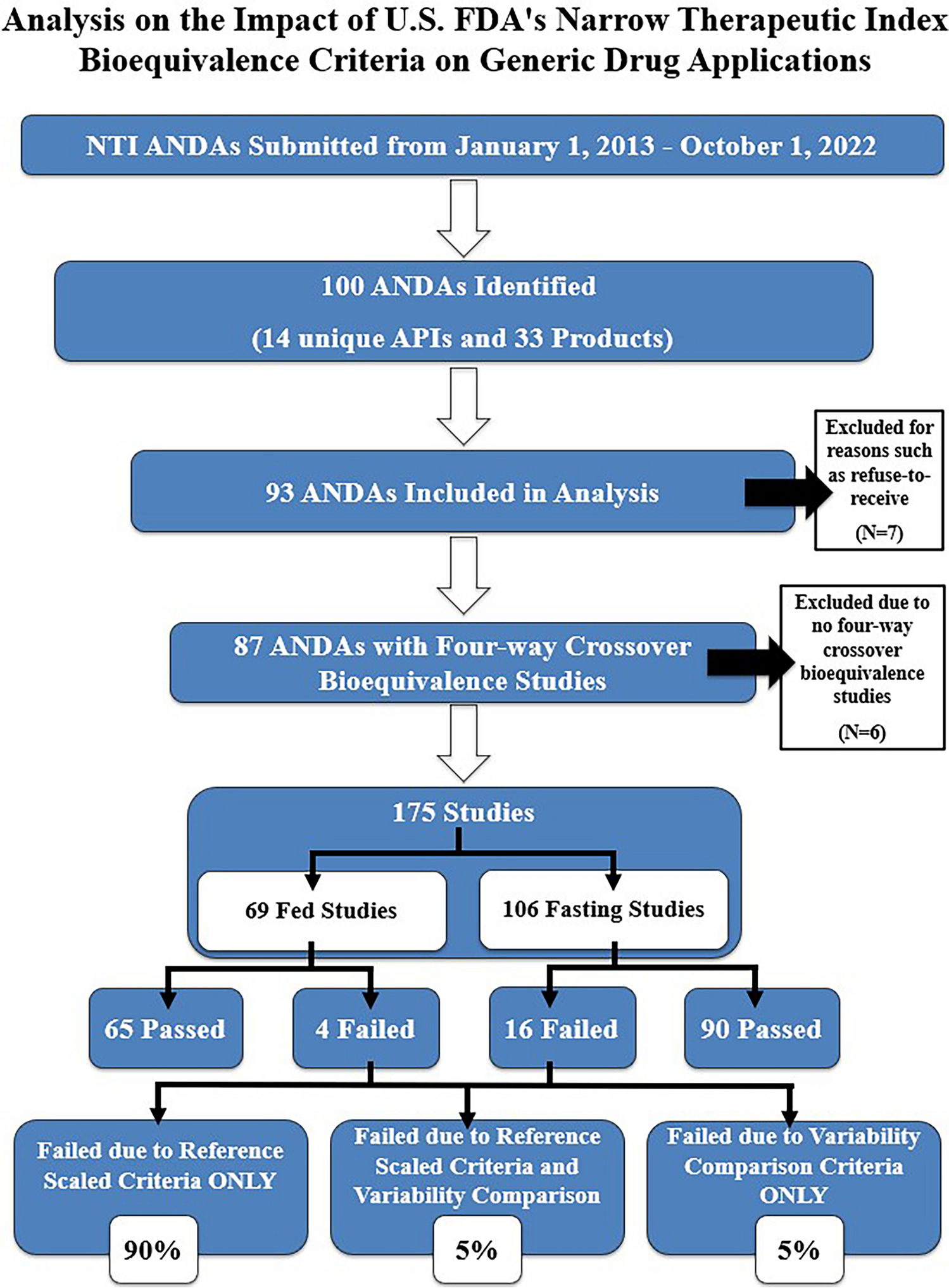

In total, 100 ANDAs for NTI drug products with initial submission dates from the FDA on or after January 2013 to October 2022 were identified (Fig. 1). Collectively, they comprised of 14 unique active pharmaceutical ingredients (APIs) and 33 drug products. Seven ANDAs were excluded due to the applications being withdrawn before the BE assessment was completed, refused-to-receive, the BE review was completed after October 1, 2022, or for other reasons. Overall, this resulted in 93 ANDAs being included in our analysis. Of the 93 ANDAs, 6 ANDAs had two-way crossover BE studies only, 10 ANDAs conducted both two-way and four-way crossover BE studies, and 77 ANDAs had four-way crossover BE studies only. Of the 6 ANDAs with solely two-way crossover BE studies conducted, 3 ANDAs had BE studies deemed adequate based on two-way crossover studies prior to their respective PSGs being updated and 3 ANDAs were withdrawn prior to approval. Among the 10 ANDAs with both two-way and four-way crossover BE studies conducted, 8 of the ANDAs were approved based on four-way crossover BE study data, 1 ANDA was withdrawn after a four-way crossover BE study was conducted, and 1 ANDA received a complete response. From the 77 ANDAs with four-way crossover BE studies only, 30 ANDAs were approved, 18 received complete responses, 9 ANDAs were withdrawn, 19 ANDAs are under review, and 1 ANDA was subjected to conventional average BE limits of 80.00–125.00%, as the PSG was updated to recommend four-way BE study criteria only after the ANDA was approved.
Fig. 1
Abbreviated new drug applications bioequivalence data collection for narrow therapeutic index drug products (2013–2022)
FDA and EMA PSG Availability for NTI Drug ProductsThere are 33 FDA PSGs for NTI drug products (14 unique APIs) recommending four-way crossover BE studies with 2012 FDA NTI BE criteria (Table I) between 2012 and 2023. All 33 PSGs recommend fasting and fed BE studies, except levothyroxine sodium whose recommended BE study is under fasting conditions only. Currently, NTI drugs are considered “high-risk”. In addition, patients may not strictly follow the labeling instructions. Thus, for these “high-risk” products, in most cases FDA recommends both fasting and fed BE studies for NTI IR drug products regardless of if labeling recommends taking with food or not. For ER products, FDA recommends fasting and fed BE studies due to concerns of dose dumping under the fed conditions. Cyclosporine IR capsule, lithium extended release (ER) tablet, phenytoin sodium ER capsule, and theophylline ER tablet have two unique PSGs for drug products that have different RLD and/or reference standard (RS) numbers but share the same API and dosage form with either different strengths and/or formulations.
Table I Narrow Therapeutic Index Drug Products and Product-specific Guidance AvailabilityEMA has six product-specific bioequivalence guidances for NTI drug products and critical dose drugs, which include: acenocoumarol tablets, colchicine tablets, everolimus tablets and dispersible tablets, levothyroxine sodium tablets, sirolimus coated tablets, and tacrolimus granules for oral suspension. Ciclosporin is also considered as an NTI drug by EMA although no PSGs was published for this drug (15). Among the six available product-specific bioequivalence guidances, they all recommend BE limits 90.00–111.11% for AUC, and standard BE limits of 80.00–125.00% for Cmax. Furthermore, FDA does not classify colchicine as an NTI product, and recommends conventional two-way crossover studies for BE demonstration of colchicine 0.6 mg oral tablet and oral capsule, respectively. For the remaining five products, FDA does consider them as NTI drugs and recommends 2012 NTI BE criteria for BE assessment. It is of note that EMA’s PSGs for acenocoumarol, colchicine, and tacrolimus recommend a fasting single-dose, two-way crossover study, while FDA’s PSG recommends both fasting and fed single-dose, four-way fully replicated crossover studies. EMA’s PSGs are consistent with EMA’s current Guideline on the Investigation of Bioequivalence, as it states in general a BE study should be conducted under fasting conditions only (16).
Analysis of Four-way Crossover BE StudiesAverage SWR of Different Narrow Therapeutic Index Drug ProductsWSV for the reference drug is an important parameter as the BE limits of NTI drugs are scaled based upon the WSV of PK parameters, as a lower WSV results in tighter BE limits with current FDA NTI BE criteria (4). In a fully replicated crossover BE study, SWR and SWT can be obtained. Thus, SWR and SWT are compared to determine whether they differ significantly. In a partially replicated crossover study with reference drug given twice and test drug given once, only SWR is obtained, therefore, no variability comparison of test and reference products can be performed with this type of study design.
Among the 18 NTI drug products with four-way crossover BE studies submitted between January 2013 to October 2022, the average SWR of Cmax and AUC (AUCt and AUCinf) per NTI product was calculated. Approximately 0.0%, 22.2%, 50.0%, and 27.8% of these products had average SWR for Cmax less than or equal to 0.05, 0.05–0.10, 0.10–0.20, and 0.20–0.30, respectively (Fig. 2). For AUC, approximately 5.6%, 22.2%, 61.1%, and 11.1% of these products had SWR less than or equal to 0.05, 0.05–0.10, 0.10–0.20, and 0.20–0.30, respectively (Fig. 2). Overall, for both Cmax and AUC, the majority of average SWR fell within 0.10–0.20, at 50.0% and 61.1%, respectively. In addition, more drug products had an average SWR less than or equal to 0.05 for AUC than Cmax, at 5.6% versus 0.0%, respectively. The distribution range of average SWR for AUC was slightly broader than Cmax, as there was one drug product with an average SWR for AUC at 0.27 compared to 0.24 for Cmax.
Fig. 2
Distribution of average SWR of various narrow therapeutic index drug products with four-way crossover bioequivalence studies
Of 14 NTI drug products with at least 4 BE studies submitted (Table III), the average SWR for AUC was between 0.06 and 0.23 and the average SWR for Cmax was between 0.10 and 0.23. For carbamazepine IR tablet, IR suspension, and ER tablet, the average SWR (standard deviation) for AUC was 0.11 (0.07), 0.06 (0), 0.19 (0.06) and average SWR (standard deviation) for Cmax was 0.10 (0.04), 0.11 (0.03), 0.18 (0.06), respectively (Table III). Divalproex sodium delayed release (DR) pellet capsule and ER tablet had an average SWR (standard deviation) for AUC of 0.06 (0.01) and 0.23 (0.09); and average SWR (standard deviation) for Cmax of 0.06 (0.03) and 0.19 (0.06), respectively (Table III). Overall, for most NTI drug products, the average SWR was below 0.21.
For products with labeling recommending taking drug on empty stomach, e.g., tacrolimus ER tablets and ER capsules, both fasting and fed BE studies were conducted. Slightly lower average SWR was observed with fed BE study than fasting BE study. For tacrolimus ER tablets and ER capsules, the presence of a meal affects the absorption of tacrolimus; the rate and extent of absorption is greatest under fasting conditions. For this reason, the labeling states that “Take once daily on empty stomach at the same time of the day, preferably in the morning.”. For products with labeling recommending drug to be taken with food, e.g., carbamazepine IR and ER tablets, both fasting and fed BE studies were conducted. There is also lower average SWR with fed BE studies than fasting BE studies.
Distribution of Passed and Failed Four-way Crossover Bioequivalence StudiesThere were 175 four-way crossover BE studies submitted (Fig. 3). In total, 89% of the BE studies passed 2012 FDA NTI BE criteria and 11% failed the criteria. Of the passed studies, 65 were fed and 90 were fasting BE studies. Among the studies that failed NTI BE criteria, 4 were fed and 16 were fasting BE studies. Of the four failed fed BE studies, two failed fed BE studies had corresponding failed fasting BE studies, both of which are IR products. Two failed fed BE studies had corresponding passing fasting BE studies, both of which are ER products. Additionally, among the failed fed studies, three studies failed due to reference scaled limits and one study failed due to variability comparison, as the test product had much higher variability than the reference product. Overall, based on all failed fasting and fed BE studies, the majority have lower within-subject variability under fed conditions.
Fig. 3
Distribution of passed and failed fasting and fed four-way crossover bioequivalence studies
As shown in Table II, 20 studies failed 2012 FDA NTI BE criteria, with 15 (16.7% of IR products) of the failed studies being for IR NTI drug products and 5 (5.9% of the ER products) being for ER NTI drug products (Table II). For the IR products which failed the NTI BE criteria, they only failed the reference scaled criterion, not variability comparison. Namely, 11, 2, and 2 BE studies failed reference scaled criterion for Cmax only, for AUC only, and for both Cmax and AUC, respectively. For the failed BE studies with ER products, 2, 1, 1, and 1 failed the reference scaled criterion for Cmax only, failed reference scaled criterion for AUC and Cmax, failed variability comparison for AUC and Cmax, and failed variability comparison and reference scaled criterion for Cmax only, respectively. Overall, about 90% of study failures are related to Cmax; 90% of study failures are related to failed reference scaled criterion. Only ER products failed variability comparison.
Table II Distribution of Bioequivalence Study Failures Among Solid Oral Immediate Release (IR) and Extended Release (ER) Narrow Therapeutic Index Drug ProductsSWR Ranges for Passed and Failed Four-way Crossover BE StudiesThe ranges of SWR among failed and passed four-way crossover BE studies were analyzed. The range of SWR for AUCt among failed four-way crossover BE studies exhibited a mean and median of 0.12 and 0.08, respectively (Fig. 4). Meanwhile, for passed four-way crossover BE studies, a slightly higher mean and median of SWR for AUCt were observed at 0.16 and 0.15, respectively. For Cmax, failed BE studies demonstrated a slightly lower mean SWR than passed studies, i.e., 0.11 vs 0.17. Likewise, for both AUCinf and AUC0–48 a lower mean and median for SWR were observed among failed four-way crossover BE studies compared to passed four-way crossover BE studies. Additionally, among passed four-way crossover BE studies, several SWR at the higher end were observed, e.g., SWR for AUCt was 0.41 in one ANDA for divalproex sodium ER tablet. However, among 11 studies submitted for divalproex sodium ER tablet, the average SWR for AUC for this drug product is 0.23. The applications that have a SWR ≥ 0.2142 are subject to BE limits of 80.00–125.00%.
Fig. 4
SWR of failed and passed four-way crossover bioequivalence studies
We further analyzed the proportion of SWR among passed BE studies for Cmax, AUCt, and AUCinf. For Cmax, there was 33.3%, 78.6%, 88.0%, 100.0%, 100.0%, and 100.0% passing rate for the SWR ranges of less than or equal to 0.05, between 0.05–0.10, 0.10–0.20, 0.20–0.30, 0.30–0.40, and greater than 0.40, respectively (Fig. 5). For AUCt, the passing rate was 100%, 73.0%, 91.0%, 96.8%, 100.0%, and 100.0% in the above ranges, respectively (Fig. 5). For AUCinf, passing rates were 100.0% for all SWR ranges except the passing rate was 75.0% and 96.8% when SWR is in the range of 0.05–0.10 and 0.10–0.20, respectively (Fig. 5). Overall, there was a higher failure rate (66.7%) for Cmax but not AUC when the SWR is less than or equal to 0.05. When SWR is between 0.05 and 0.10, approximately 75% of all PK parameters passed the NTI BE criteria (Fig. 5).
Fig. 5
Proportion of SWR per pharmacokinetic parameter for passed bioequivalence studies
Comments (0)