
Remember me
Fundamentally, the medical education system exists to generate the health care workforce. It is our goal as educators to prepare our learners for the health system in which they will practice. Despite an intellectual recognition of the inter-dependence between health care delivery and health professions training [1], this connection can be lost in the day-to-day process of education. This is particularly true in the United States (US). Given our strong orientation to individualism, education risks becoming transactional. Leaders of educational programs are vulnerable to focusing on learners’ career aspirations, promising a competitive advantage for the next stage of training. Learners, in turn, behave in accordance with the systems we have created. Our historical normative orientation inadvertently breeds perverse incentives for learners to pursue metrics of “merit” that are often not aligned with meeting the needs of the communities they will ultimately serve, such as over-emphasis on standardized testing or prioritizing early publication opportunities over patient-facing experiences [2]. A successful and principled senior medical student I once worked with lamented “Med school is less about becoming a good doctor and more about compiling a competitive resume.” Given the median medical school debt among those reporting debt (68% of respondents) is $200,000 [3], it is not surprising that students would be strategic about their advancement. Applying a systems perspective encourages us to step back and take a broader view. Systems thinking—“a holistic approach to understanding a system’s component parts, and the interrelatedness of these parts, to better understand how a system works and evolves over time” [4]—can empower educators to manage the rapidly evolving societal context in which we collectively work and learn.
Creative innovators in health science education have tackled the issues raised above, intentionally or fortuitously demonstrating habits of systems thinkers [5] in the process. Many basic science educators have contributed to re-orienting curricula around organ systems, driving integration across content domains and facilitating learners’ appreciation of foundational sciences in a clinical context. Pass/fail grading has been implemented with hopes of fostering a growth mindset and reducing unproductive stress. Progress in implementing competency-based medical education, which anchors the educational program around the needs of patients and communities, has fostered articulation of performance criteria that provide clearer developmental guidance than traditional normative rankings. A philosophical shift from “sage on the stage” to “guide on the side” engages our talented adult learners as colleagues, fostering agency and professional identity formation. Efforts to integrate scientific foundations into advanced clinical experiences can be more challenging, but successful strategies have emerged [6]. The team-based teaching and faculty engagement that underpins all these innovations role model the teaming and continuous improvement that will be necessary in learners’ future clinical practice.
Our education community is now faced with a major disruptor: artificial intelligence (AI). The Global Forum on Innovation in Health Professional Education, sponsored by the US National Academies of Sciences, Engineering and Medicine, identified AI as an urgent issue for educators in 2020, published a call to action in 2021 [7], and conducted a public workshop in 2023 [8]. This message initially met resistance from the education community, with claims that the topic is too futuristic, AI is too imperfect, the curriculum is too full. Now, the prevalence of tools such as Chat GPT has forced engagement. We must change perspectives to envision the future of both practice and learning. The American Medical Association has espoused the term “augmented intelligence,” focusing on “AI’s assistive role, emphasizing that its design enhances human intelligence” [9]. The best outcomes will occur when professionals (human intelligence) leverage artificial intelligence to augment our performance, while maintaining our duty as advocates for learners, patients, and communities. This is the world for which, and in which, we must prepare our trainees.
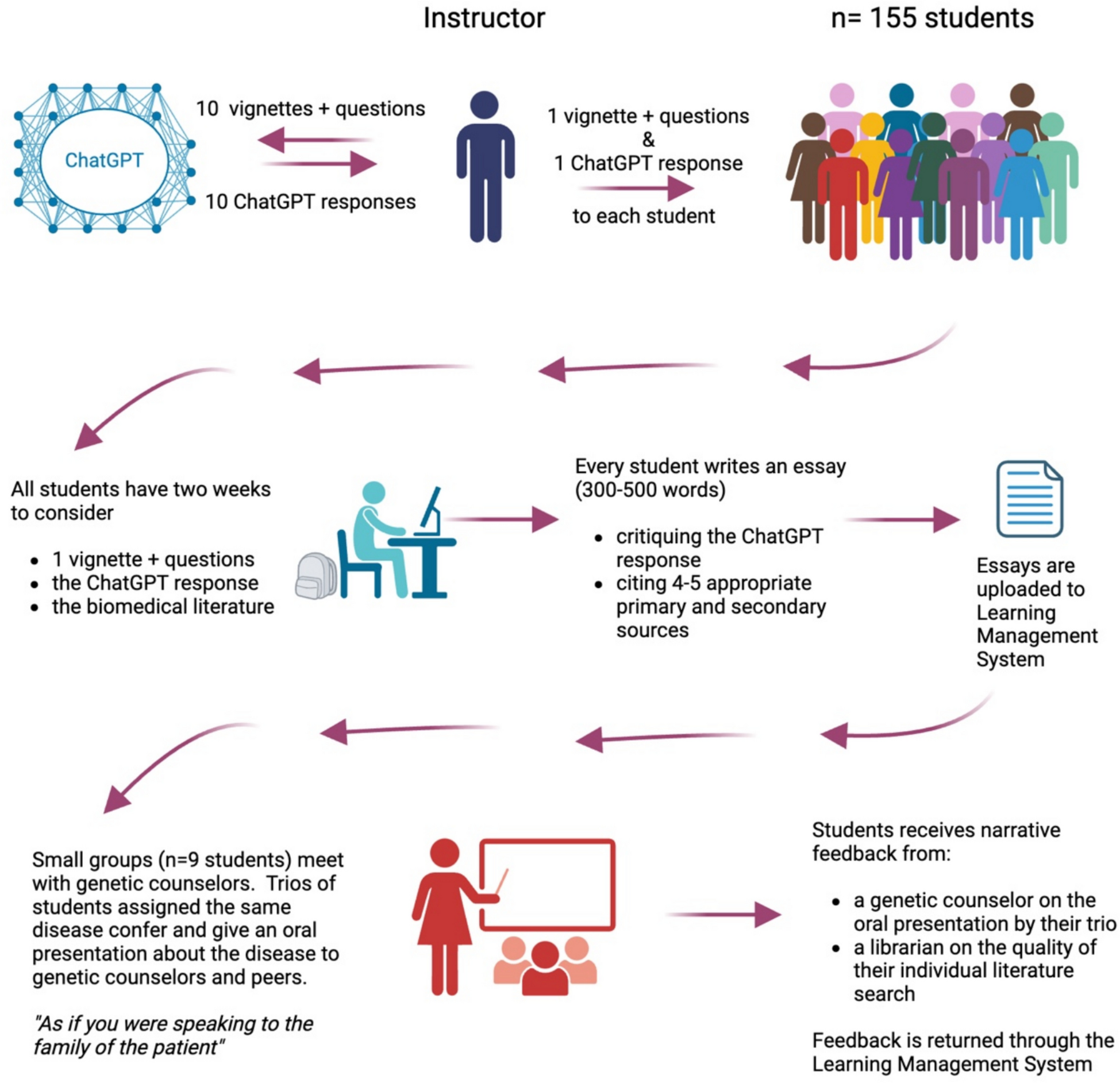
Educators must consider (1) what skills in AI health professionals will need to deliver care and (2) how AI can be applied to improve our processes of education. How can a systems approach empower educators in this work? An illustrative common impulse among educators facing the rapid proliferation of AI tools is to fear that students will use AI to “cheat.” It is valid to acknowledge that such technology strains our current structures and to adjust accordingly but banning the use of AI is not productive to preparing learners for their future. A systems approach encourages us to reconsider our mental models, enabling us to align education with the demands of the rapidly evolving health system. Rather than decry student utilization of generative AI to draft essays, the systems-thinking educator flips perspectives, inviting students to use AI for a first pass and requiring them to do the deeper cognitive work of analyzing the quality of the resulting output. This creative educator converts the essay to an opportunity to illustrate the power and limitations of AI while concomitantly driving a deeper response to the primary learning objective. Educators must actively nurture transparency, human agency, and critical appraisal, all essential duties of health professionals in the safe implementation of AI in the care of patients and populations.
Viewing medical education as a complex system guides improvement. In the realm of health care delivery, the Institute for Healthcare Improvement’s Triple Aim (improving health outcomes, improving the patient’s experience, and reducing cost) has been expanded to the Quintuple Aim to include protecting the well-being of the health care workforce and advancing health equity. Our educational system needs analogous improvements (Fig. 1). Artificial intelligence may assist educators in achieving our aims of improving learning outcomes, enhancing each learner’s experience, reducing the cost of education, protecting educators and the education mission [10], and enhancing equity in our education processes.
Fig. 1
The educational equivalent of the Quintuple Aim
Precision education [11]—leveraging data and technology to make education more personalized, relevant, and efficacious—is an ambitious vision for driving such improvement in our education systems. One example of applying precision to improve learning outcomes lies in the longstanding observation by basic science educators of differing competency needs among early learners: some need more assistance in developing core knowledge, while others require development in teamwork or communication skills. Historically, however, pre-clinical assessments are limited regarding learner performance in domains other than medical knowledge, making it difficult for those educators to justify tailored actions. AI tools such as natural language processing can be applied to narrative comments from small group facilitators, peers, and clinical supervisors to integrate sporadic feedback across courses and settings, illustrating via digital dashboards actionable competency trends in diverse domains. Similarly, clinical work artifacts of students, residents, and practicing physicians—such as encounter notes and orders—can be analyzed using AI applications to catalog clinical activities (concomitantly identifying gaps in required clinical exposures), provide prompt feedback regarding foundational knowledge and clinical reasoning, and guide future learning. Increasingly, educators will have data and tools to customize training to one’s learning needs, hopefully combating the often-dehumanizing effects of medical training by assuring learners they are seen and supported as individuals.
Technology alone will not produce the system to which we aspire. Education is fundamentally a social process, anchored in relationships and organizational context. Educators thrive on relationships; helping our trainees achieve their goals is deeply rewarding. Those relationships, however, are strained when learners feel compelled to conceal their own uncertainties. Continued attention to the learning environment is critical to foster a developmental mindset and support the Master Adaptive Learner throughout a health professional’s career [12]. The successful health professional of the future is not the individual “possessing” the most knowledge, but rather the individual embracing epistemic humility [13] who poses the best questions, taps into collective intelligence, and critically applies knowledge appropriately to each patient. We must create the deliberately developmental organizations14 in which such behaviors are fostered and valued. Contemplating the broader impact of AI at the intersection of systems of health care delivery and health professions education will position innovative educators to radically rethink what we teach, how we teach, and even whom we teach.
The disruptive force we face, and the work ahead to respond to it, is simultaneously daunting and exhilarating. By explicitly testing our own assumptions about how and what one should learn, and collaborating across our community, educators will be empowered to lead transformation. Systems thinking will help us apply levers to preserve what we value most: ensuring our learners are well-positioned to thrive in service to patients and communities.
Comments (0)