
Remember me

The increase of the robotic liver surgery (RLS) approach is exponential, at the expense of a decrease in the laparoscopic liver surgery (LLS) approach, which since 2018 has experienced a decline in the number of resections worldwide [1]. This increase has been parallel to a very notable growth of the companies dedicated to the manufacture and development of surgical robots, with high revenues only in 2022, as disclosed i.e., by Intuitive® (6.2 billion dollars), CMR surgical® (450 million dollars), or Medtronic® surgical innovations (1.5 billion dollars).
The RLS reports have described a refinement in progressively complex procedures, while showing results financially comparable to open resections [2], including major, anatomic, donor, and complex liver resections, supporting the hypothesis of being a reproducible, safe approach, with an increasing technical ceiling [3], and a faster learning curve compared to the laparoscopic approach [4], which may allow moving to robotic from the open approach with no need for a previous full laparoscopic learning curve.
In the pan-European survey on the implementation of robotic and laparoscopic minimally invasive liver surgery [5], only 28% of surgeons surveyed reported performing major procedures, and 29% minor, and up to 46% described their method of liver transection with the use of bipolar forceps, omitting the CUSA. Although 30% of surgeons stated they prefer robotic surgery, they expect an increasing implementation of RLS in the future, admitting it could be more expensive than LLS.
Several consensus has giving the LLS a wide acceptance and a high recommendation degree, such as the Louisville [6] and Morioka declarations [7], the International Liver Laparoscopy Society [8], the Southampton Guidelines [9], or the Consensus Guidelines [10], while classifying the RLS as non-inferior approach, mainly due to the lack of high-quality evidence.
Despite this, it is accepted that the RLS is superior by providing an expanded three-dimensional 3D stereo vision, ergonomic station, very good bipolar and monopolar energy, enhanced flexibility (thanks to the 7 degrees of movement of the robotic arms), and tremor filter (useful to perform fine dissection of vital structures and sutures in narrow space), helping to overcome the shortcomings experienced in conventional LLS.
The technical developments of RLS had boosted its use in the clinical practice, as well as the international series reports [11, 12]. The international consensus statement on RLS also contributed to its standardization [13]. Furthermore, some important issues, such as the cost-effectivity or cost-efficiency results remain controversial.
Methodologically, RLS has been developed from the LLS lessons learned, such as the caudal approach for the hilar plate [14], the Laennec capsule for the “liver gates” [15], and the “cone units” [16], improving the anatomical precise and parenchyma-preserving resections.
Technically, the robot introduces several innovative features that favors the intraoperative navigation, such as the integrated in-console vision of the intraoperative ultrasound, and the simple switch to indocyanine green (ICG) vision for the negative and positive parenchyma staining [17, 18], but also the virtual 3D model assistance [19], and identification algorithms [20]. That is why, the RLS is currently in stage 2a of the IDEAL development framework of surgical innovations [21] (equivalent to pioneer surgeon), while the LLS is in stage 3, close to stage 4 (“early adopter” for many centers, but being established practice in others).
Notwithstanding, the available instruments for liver parenchymal transection (LPT) are limited, as the robot do not offer the tools former established for open and laparoscopic LPT, such as the cavitronic dissector, the harmonic sealer, or the radio-frequency coagulator. That is why the absence of a systematized technique has led to the development of several options for LPT, which in many cases have become standard in each institution.
This variability in the LPT technique is the origin of a controversial widespread heterogeneity, that significantly limits the overall analysis of the technical ceiling of the robotic approach, making it difficult to assess the cost associated to liver resections.
Robotic LPT can be performed under three modalities, regarding the current state-of-the-art:
Robotic Assisted, when the scrubbed assistant surgeon transects the liver parenchyma with a laparoscopic tool that is foreigner to the robot system, but under robotic assistance, i.e., laparoscopic cavitron ultrasonic surgical aspirator [22,23,24,25], or waterjet [26].
Totally Robotic, using advanced robotic tools, such as the Vessel Sealer [27], the Harmonic Scalpel [28,29,30], the SLiC saline-linked electrocautery [31], or the Synchroseal [32].
Real Robotic, with no use of laparoscopic or robotic advanced tools, using only plugged bipolar fenestrated forceps, bipolar Maryland forceps, monopolar curved scissors, or monopolar permanent cautery spatula.
As no robotic platform includes the specific standardized tooling for LLS, it can be stated that the minimal common LPT technique option has to be based upon the use of the tools offered as standard by the platform (basically forceps and scissors), along with the selective use of the bipolar and monopolar energy, respectively, in order to progress into the transection plane through small steps we may call “microfracture-coagulation” (MFC).
The first reports of the real robotic LPT were described as “crush-clamp” technique variants, with the use of bipolar energy devices [33,34,35], but the MFC method has not been yet systematized.
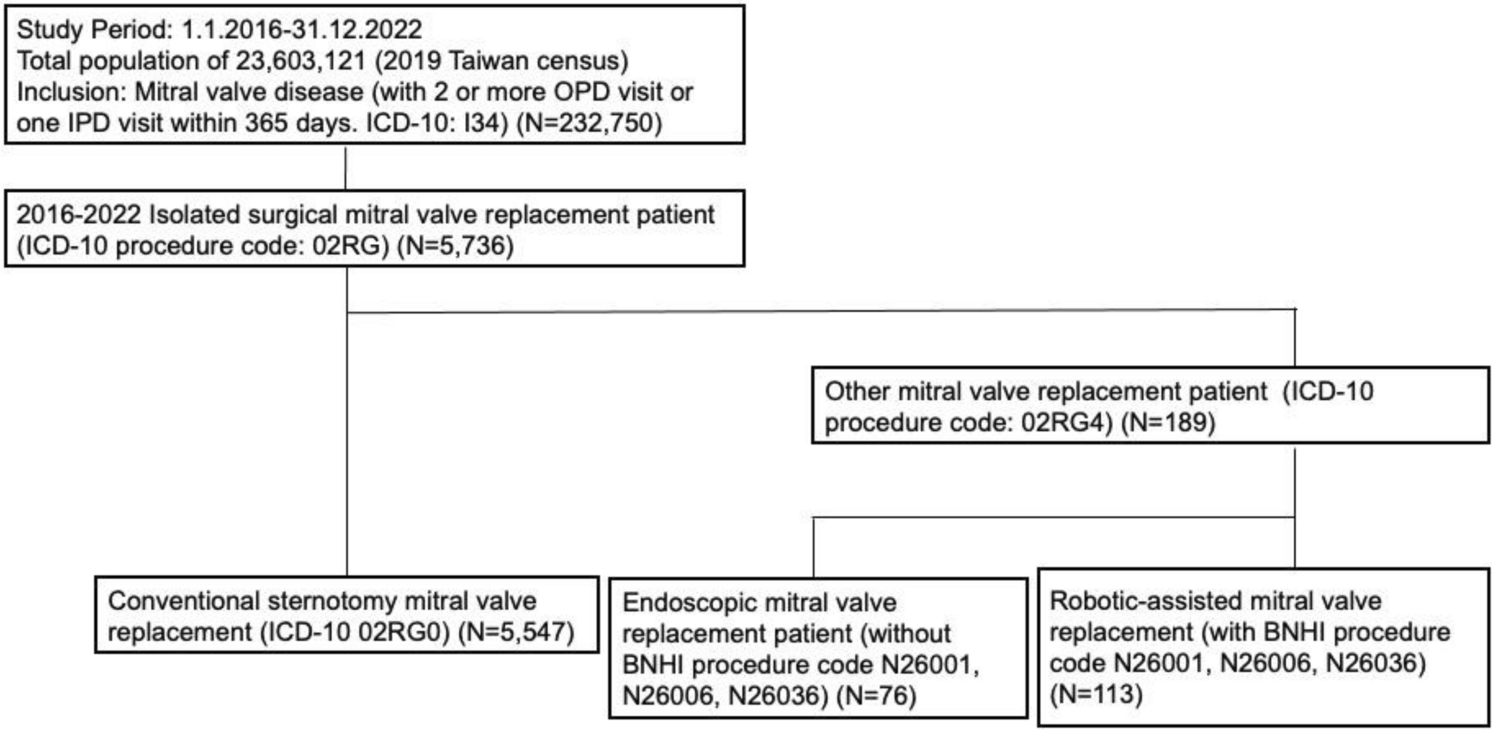
This technique is systematically used in all RLS cases at our institution since 2018 [36]. The series (Table 1) includes 131 robotic liver resections for 138 lesions, performed in 123 patients with the Da Vinci Xi Surgical System, consecutively collected between April 2018 and October 2023. Patients were aged 63.7 (20–82) years, mainly men (53.7%), with median BMI 27.7, and median Charlson comorbidity index 7.1. Main indication was malignancy (74.8%). Surgical resections were predominantly anatomical: 83 cases (67.5%), including major hepatectomies (10.7%) and two-stage hepatectomies (2 ALPPS cases). There were 66 cases of lesions in posterior segments 6,7,8 (42.5%), considered difficult in LLS. The mean operative time was 217.6 min, with a Pringle hilar clamping time of 50.9 (17–123) min. The mean blood loss was 168.1 ml, and 4 patients received perioperative transfusion. The median total hospital stay was 4.2 days. Morbidity before 90 days postoperatively Clavien-Dindo ≥ grade 3 in 6 cases (4.9%), with 3 ISGLS B/C bile leaks, and 3 cases of conversion: 1 to laparoscopy (irreversible energy failure) and 2 to open surgery (adhesion syndrome, and hidden bleeding point check after procedure). There was 1 case of re-intervention (laparoscopic intestinal lesion prior to docking), and 1 case of mortality (ISGLS grade 3 irreversible postoperative liver failure after anatomical resection of segment 8 in a Child B cirrhotic patient).
Table 1 Sample series. Baseline characteristics and perioperative detailsSurgical techniqueIndicationsMFC is indicated in any type of robotic liver resection, from minor to major, and from parenchyma-sparing to enlarged anatomical liver resections, including complete piggy-back/ hanging maneuver and two-stage liver resection.
Technical descriptionMFC for real robotic LPT can be defined by the simultaneous and synchronized use of the EndoWrist bipolar fenestrated forceps and the EndoWrist monopolar curved scissors, both plugged into the integrated ERBE VIO dV 2.0 generator cut and coagulation (effect 6), usually under extracorporeal Pringle hilar clamping.
The patient positioning (Fig. 1) is supine decubitus open-legged, with the arms closed, with 8° anti-Trendelemburg, above body vacuum mattress. The position may be modified with the integrated table position at will during the procedure, although left decubitus may be used for true right posterior lesions resections.
Fig. 1
Patient positioning. (a) Supine decubitus open-legged French position with 8° anti-Trendelemburg for anterior lesions. (b) Left decubitus for right posterior lesions
The 4-trocar placement (Fig. 2) follows a horizontal line above the umbilicus, leaving bipolar forceps left to the camera trocar, and monopolar scissors right to it, leaving the fourth trocar free for liver mobilization and traction. Depending on the body mass index, the fourth trocar may be placed slightly upper from the trocar baseline. The right tool trocar (usually nº 3, is a 12 mm trocar with 12–8 mm reducer cannula to admit EndoWrist SureForm 60 mm and 45 mm curved-tip endostaplers). One assistant trocar may be placed below, 7 cm equidistant from the camera trocar and the curved scissors trocar, to irrigate/suction, or to provide material supply, as gauze or stitches, as needed. The trocar placement for left decubitus follows the same disposition, but leaving the subcostal anterior axillary point for trocar 2 pointer. The hilar Pringle clamping is extracorporeal with a Rommel tourniquet using a 24FR Nelaton catheter through a 5 mm left incision for right liver lobe lesions, but right for left lobe lesions.
Fig. 2
Trocar placement. (a) Supine decubitus for anterior lesions. Trocar placement above the umbilicus (1: Fenestrated forceps port, 2: Pointer and camera port, 3: Curved scissors trocar, R: 12–8 mm reducer cannula, A: Assistant 12 mm laparoscopic trocar); (b): Left decubitus for right posterior lesions. Subcostal trocar placement
The Glisson capsule is incised with the curved monopolar scissors, making a 1–2 cm fence along the desired transection line, once the navigation tools are checked in-console (i.e., intraoperative ultrasound, ICG dye staining, or 3D model consultation).
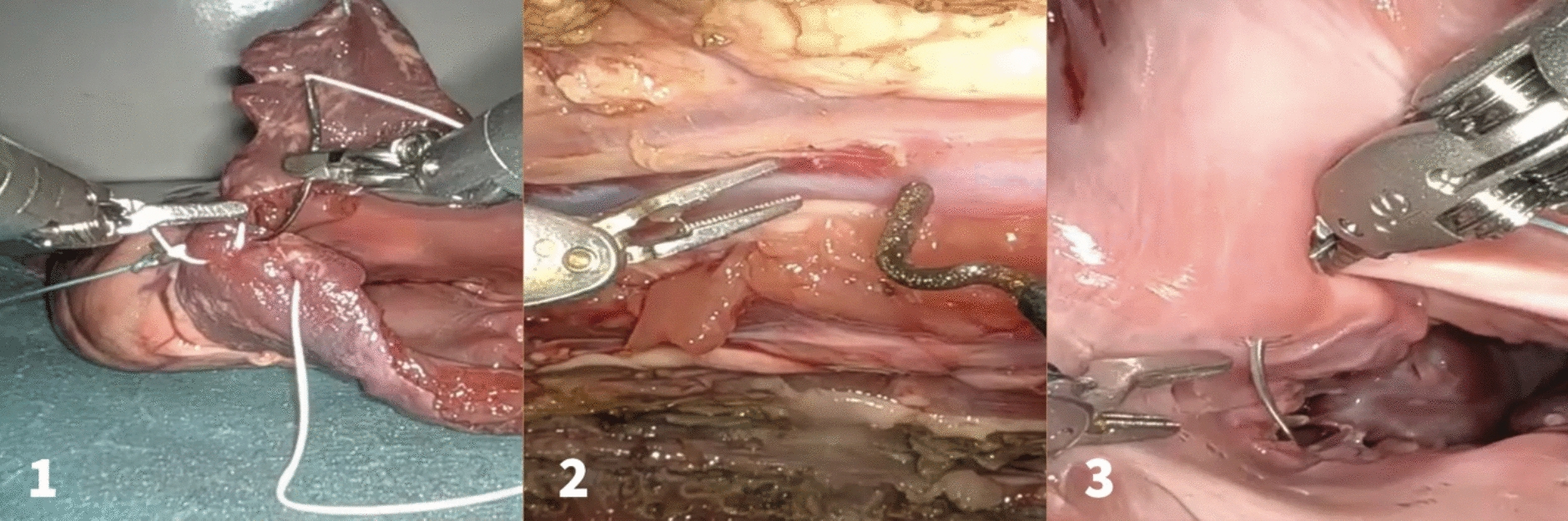
The method of progression during the LPT is subdivided into three consecutive steps, as follows (Fig. 3):
Fig. 3
Microfracture-coagulation steps. (a): First step cold progression. Initial position; (b): First step cold progression. Final position after microfracture; (c): Bipolar and monopolar energy coagulation
1-First step: Cold progression, starting in contact with the transection cutting surface, where the separation of the tooltips fractures the parenchyma towards deep, thus carefully revealing the anatomy of the communicating vessels and the 3rd order glissonian and main hepatic vein branches. The EndoWrist monopolar curved scissors may dissect the vessel and surround it 360º to obtain a security stump after cutting.
2-Second step: Bipolar energy application, in which the bipolar forceps coagulates the selected vessel (up to 5 mm) by diathermy, before cutting it with monopolar energy with the scissors.
3-Third step: Monopolar energy application, in which the monopolar curved scissors coagulates the new transection frontline before proceeding to repeat the series.
Vessels up to 15 mm may be isolated by cold dissection in a segment wide enough to apply medium-large locked clips with the robotic applier, prior to section it with scissors, while first and second order glissonean pedicles may be identified without being injured, dissected, surrounded with a loop with the wristed forceps, and lift it up, thus allowing the progress of the wristed robotic endostapler for mechanical transection, with SureForm wristed da Vinci blue reload 45–60 staplers. Main hepatic veins root dissection may be transparenchymatous during major hepatectomies, and transected with tipped 35 white reload stapler.
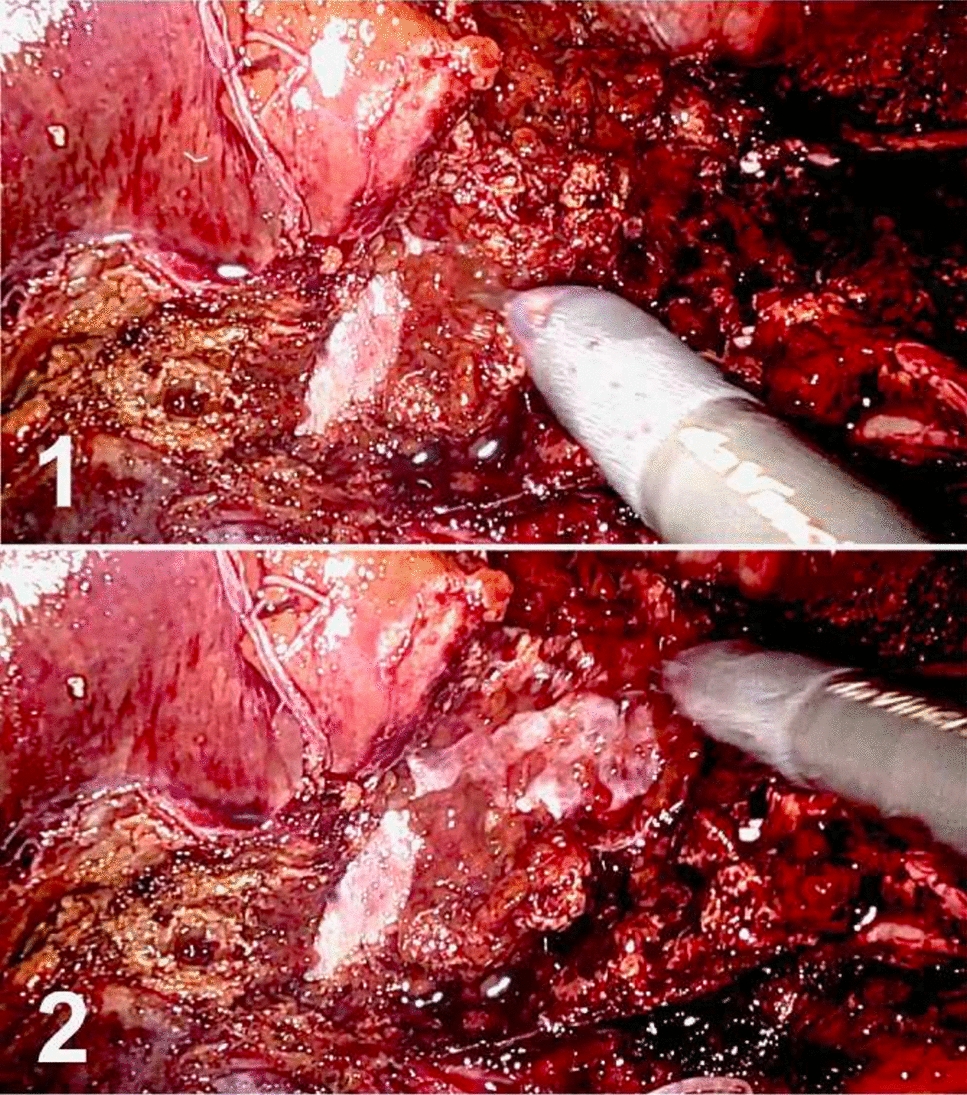
The final transection surface is checked at the end of the procedure (Fig. 4). This revision is usually done after releasing the hilar clamp, by applying gauze onto the transection surface, and then removing it rolling over, uncovering one by one the potential oozing points, so superficial bipolar coagulation can be applied selectively, avoiding monopolar coagulation that could leave ischemic bedsores areas below, and eventually be the origin of potential bilomas or hematomas.
Fig. 4
Microfracture-coagulation. (a): Final transection check. (b): Superficial bipolar coagulation is applied
Comments (0)