After the publication of several trials showing that laparoscopy offered similar oncological outcomes for improved recovery outcomes for minimally invasive right hemicolectomy [1,2,3,4,5], laparoscopy has become the standard approach for performing the procedure [6,7,8]. Nowadays, laparoscopic right hemicolectomy consists mostly in laparoscopic mobilization of the colon, extra-corporeal vessel division and lymphadenectomy (at least at the level of the ileo-colic vessels), extra-corporeal anastomosis and extraction through the midline [6, 9, 12, 14, 15, 21,22,23,24]. However, fully minimally invasive right hemicolectomy should theoretically include intra-corporeal vessel division, lymphadenectomy and anastomosis, allowing to use a C-section as extraction site. Such a procedure is possible by laparoscopy, but not universally adopted, because of the technical limitations of laparoscopy. On this aspect, robotic platforms, which offer improved minimally invasive possibilities, may allow optimizing the technique for right hemicolectomy and reaching better post-operative outcomes.
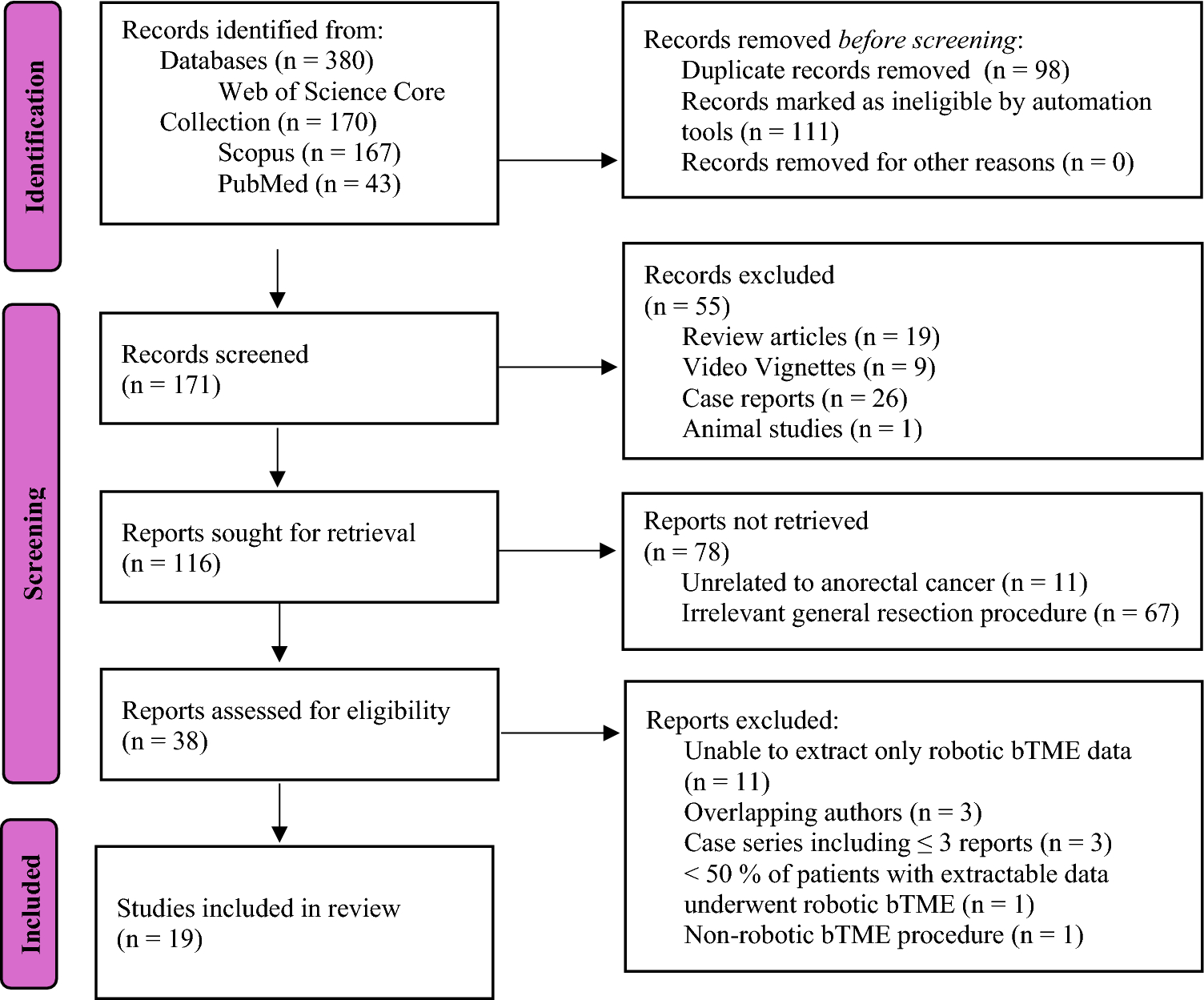
In a systematic review of the literature in the field, we identified 16 publications comparing laparoscopic right hemicolectomy with robotic right hemicolectomy [6, 8, 9, 27,28,29,30,31,32,33,34,35,36,37,38,39]. These publications showed that patients who undergo robotic right hemicolectomy have decreased blood loss, decreased incidence of post-operative complications, shorter recovery of bowel function, fewer conversions to open surgery and shorter length of stay, at the cost of a slightly longer operative time when compared to laparoscopy [41,42,43,44]. The improved post-operative outcomes observed with robotics may be explained by the facilitated realization of intra-corporeal anastomosis when compared to laparoscopy. For instance, a few publications reported that the proportion of patients who received intra-corporeal anastomosis was increased with robotics when compared to laparoscopy [12, 21, 38, 39, 45]. In the only randomized controlled trial published in the field, the proportion of intra-corporeal anastomosis was of 85.7% in patients undergoing robotic right hemicolectomy versus 20% in patients undergoing laparoscopic right hemicolectomy [38]. As a corollary, a C-section may have been chosen as the preferential extraction site in these patients, as it is the case in 77.6% of patients (98.7% for off-midline extraction site) undergoing intra-corporeal anastomosis when compared to 0% of those undergoing extra-corporeal anastomosis [24]. Noteworthy, in the MIRCAST study, extraction through a C-section was more often done in patients who underwent intra-corporeal anastomosis (odds ratio: 165.7, p < 0.001) [39]. However, the vast majority of these publications were not devoid of potential bias, as they reported the results of observational studies, included heterogeneous populations of patients and compared heterogeneous surgical techniques including or not intra-corporeal anastomosis, D3 lymphadenectomy and/or complete mesocolic excision. For instance, D3 lymphadenectomy was more often performed in the robotic group in the MIRCAST study (odds ratio: 4.22, p < 0.001) [39], which may increase the operative time of the technique and prevent any objective comparison with laparoscopy. Moreover, the majority of included studies were of limited sample sizes, were based on database analysis and/or on non-randomized data. Therefore, high-quality randomized evidence is needed to validate the findings of these early observational studies.
To date, only one randomized controlled trial compared robotic right hemicolectomy with laparoscopic right hemicolectomy [38]. In this trial, no difference was found in terms of time to first passage of flatus, length of stay, complications, postoperative pain and number of harvested lymph nodes between the two surgical techniques. Long-term analysis of the data showed similar long-term survival between the two techniques [46]. However, one main limitation of this trial was represented by the fact that the anastomosis technique was not standardized between the surgical approaches: patients who underwent robotic right hemicolectomy could receive either intra-corporeal or extra-corporeal anastomosis. Therefore, the potential main advantage of the robotic approach, which is intra-corporeal anastomosis [44], was not properly evaluated. It should, however, be noted that intra-corporeal anastomosis was more often performed in patients who underwent robotic right hemicolectomy than in patients who had laparoscopic right hemicolectomy, meaning that robotic right hemicolectomy facilitated the realization of intra-corporeal anastomosis. This assertion was confirmed by a systematic review and meta-analysis [44]. Moreover, the trial was powered on the length of stay, which was longer than nowadays standards and longer than our own personal experience with robotic right hemicolectomy, which is of 5.4 ± 3.8 days (unpublished data), and therefore, limits the validity of its findings. Finally, the total sample size was of 70 patients, which may have been insufficient to show a potential difference between groups for several of the assessed variables (type II statistical error).
From a personal point of view, we believe that the true benefits of robotic right hemicolectomy can only be only achieved when opting for a fully minimally invasive robotic approach including intra-corporeal anastomosis. A propensity score-matched analysis of 192 patients who underwent either totally robotic right hemicolectomy (including intra-corporeal anastomosis) or robotic-assisted right hemicolectomy (including extra-corporeal anastomosis) showed that improved post-operative outcomes were reported when using the totally robotic approach, in terms of post-operative pain and recovery of bowel function [47]. In a prospective cohort study of totally robotic right hemicolectomy [48], we showed that intra-corporeal anastomosis was achievable in all patients, with a low conversion rate of 3.3% and a reasonable mean operative time of 200.4 ± 114.9 min (which has to be compared to operative times up to 279 min [33] and 327.5 min [49] documented in the literature). Moreover, we reported a mean number of harvested lymph nodes of 22.4 ± 7.6, a mean length of stay was of 5.4 ± 3.8 days, a post-operative morbidity of 11.7% and no mortality. However, we note that a national audit showed that intra-corporeal anastomosis is still not routinely performed during robotic right hemicolectomy [6]. Moreover, this approach has to be compared to the actual standard of care, which is laparoscopic right hemicolectomy with extra-corporeal anastomosis, and additional longer term outcomes remain to be evaluated, such as the incidence of incisional hernia (which is modulated by the choice of extraction site). The experience of the operating surgeon on a robotic platform should also be sufficient, as it was shown that the operative time and the incidence of conversion to open surgery were inversely correlated to the personal caseload [50]. To conclude, systematic review of existing studies, which are mostly non-randomized, suggest that robotic surgery may offer improved post-operative outcomes after right hemicolectomy when compared to laparoscopic surgery, notably by facilitating the realization of intra-corporeal anastomosis and off-midline extraction of the operative specimen, as well as extended lymph node dissection. Results of ongoing randomized controlled, such as the PRORHEM trial or the ROLACART-1 pilot trial are awaited for confirming these results.


Comments (0)