In the light of increasing antimicrobial resistance, rational dosing of the currently available antibiotics is essential to preserve their activity. For antibiotics with time-dependent bactericidal killing patterns and absent or short persistent effects like many β-lactams, prolonged infusion strategies rather than dose increases have been recommended to better meet ƒT>MIC targets and to ultimately improve outcome, particularly for agents with a short half-life [21, 22].
The current analysis systematically compared the single impact of all three basic principles of dosing, i.e. infusion duration, dosing interval and TDD, on ƒT>MIC and PK/PD target attainment using the example of the β-lactam antibiotic ceftaroline. The analysis was motivated by the separate approval of a ‘high-dose’ regimen for CPT-F, which involves the intensification of all three dosing variables simultaneously, i.e. a combination of prolonged infusion duration, shorter dosing interval and enhanced TDD compared with standard dosing. The study demonstrated that the importance of each dosing component, i.e. its contribution to overall ƒT>MIC after intensified dosing, changes with decreasing susceptibility (i.e. higher MIC).
For susceptible S. aureus strains with MIC ≤1 mg/L, shortened dosing intervals (q12h→q8h) appeared primarily responsible for the high ƒT>MIC following the approved intensified dosing regimen. Prolonged infusion durations (1 h→2 h) increased ƒT>MIC even for resistant strains with MIC = 8 mg/L, but only in the case of sufficiently high doses (≥600 mg). This result is not surprising given that longer infusion durations cause lower maximum (‘peak’) concentrations, which become more relevant for ƒT>MIC at high MIC values.
Importantly, the higher the MIC (>1 mg/L), the more crucial the administered dose amount becomes. For highly susceptible strains, shorter dosing intervals and prolonged infusion durations might even suggest lower than traditional TDDs to reach a specific PK/PD target (although caution has to be exercised in clinical practice before lowering doses, particularly in patients with severe infections). However, for less susceptible strains, shorter dosing intervals and prolonged infusion durations might require higher TDDs to reach the same target. These findings are particularly relevant in the light of the increasing application of prolonged infusions up to continuous infusion of antibiotics, which entails maximum infusion duration and minimum dosing interval. Particularly when switching to a prolonged infusion and/or shorter dosing interval, a simultaneous dose increase should be borne in mind to improve target attainment given known or suspected low bacterial susceptibility. The results also call to mind the importance of considering the susceptibility of the infecting pathogen (and potential variability in MIC) for dosing, which in clinical practice however is commonly not available for healthcare providers.
Our study investigated clinically relevant MIC values up to 8 mg/L. S. aureus with MIC ≤1 mg/L represent the most common strains in Europe (MIC90 = 1 mg/L) and are classified as susceptible to CPT irrespective of its indication (S ≤1 mg/L) [14]. Tallying with this, target attainment rates were high (100%) for MIC = 1 mg/L in the study population. MIC values of 2–4 mg/L are classified resistant according to EUCAST (pneumonia: R >1 mg/L, indications other than pneumonia: R >2 mg/L) [14]. While these are rather rare in Europe, they are more prominent in Latin America and the Asia-Pacific region [23,24,25]. The intensified dosing regimen that has been approved specifically for cSSTI infections caused by S. aureus of MIC 2–4 mg/L was the only dosing strategy leading to sufficient target attainment for MIC = 4 mg/L in the investigated healthy population, highlighting its usefulness. For MIC = 2 mg/L, the PK/PD target was also met by 90% of the population after standard dosing. In cases where severely ill patients display lower antibiotic exposure than healthy volunteers (e.g. as frequently observed in sepsis), the intensified dosing regimen seems more beneficial than standard dosing for MIC = 2 mg/L.
S. aureus with MIC = 8 mg/L is classified as resistant and has rarely been identified in Europe [13, 14]. Nevertheless, MIC = 8 mg/L was included in the analysis as a worst-case scenario and to show target attainment for the full distribution of observed MIC values in Europe [14]. Our analysis suggests that a TDD of 1800 mg would not suffice to achieve a 2-log reduction of such isolates, and even higher doses might be required. However, CPT-F is not approved for the treatment of infections caused by S. aureus with MIC = 8 mg/L, and caution has to be exercised when interpreting target attainment for MIC = 8 mg/L as the target ƒT>MIC = 35% had been determined based on an upper MIC = 4 mg/L [17].
The target ƒT>MIC = 35%, indicating a 2-log10 CFU reduction of S. aureus, was exemplarily chosen in our analysis. We aimed for the most conservative available PK/PD target for ceftaroline against S. aureus, reflecting a 2-log10 CFU reduction, rather than a target reflecting bacteriostasis (ƒT>MIC = 26.8% [17] or ƒT>MIC = 20.3% [13]) even in the healthy study population. In clinical practice, the PK/PD target underlying dosing decisions might differ, e.g. depending on the patient’s clinical condition. For example, stricter PK/PD targets such as ƒT>MIC = 100% have been suggested for β-lactams, especially for intensive care unit (ICU) patients with severe infections [26]. PK/PD targets might also vary for different types of infection and antibiotic agents (even within a β-lactam class). However, the general trends in target attainment across systematically varied dosing regimens and MIC values are likely similar to those illustrated for other antibiotics with PK/PD characteristics and half-life comparable to CPT.
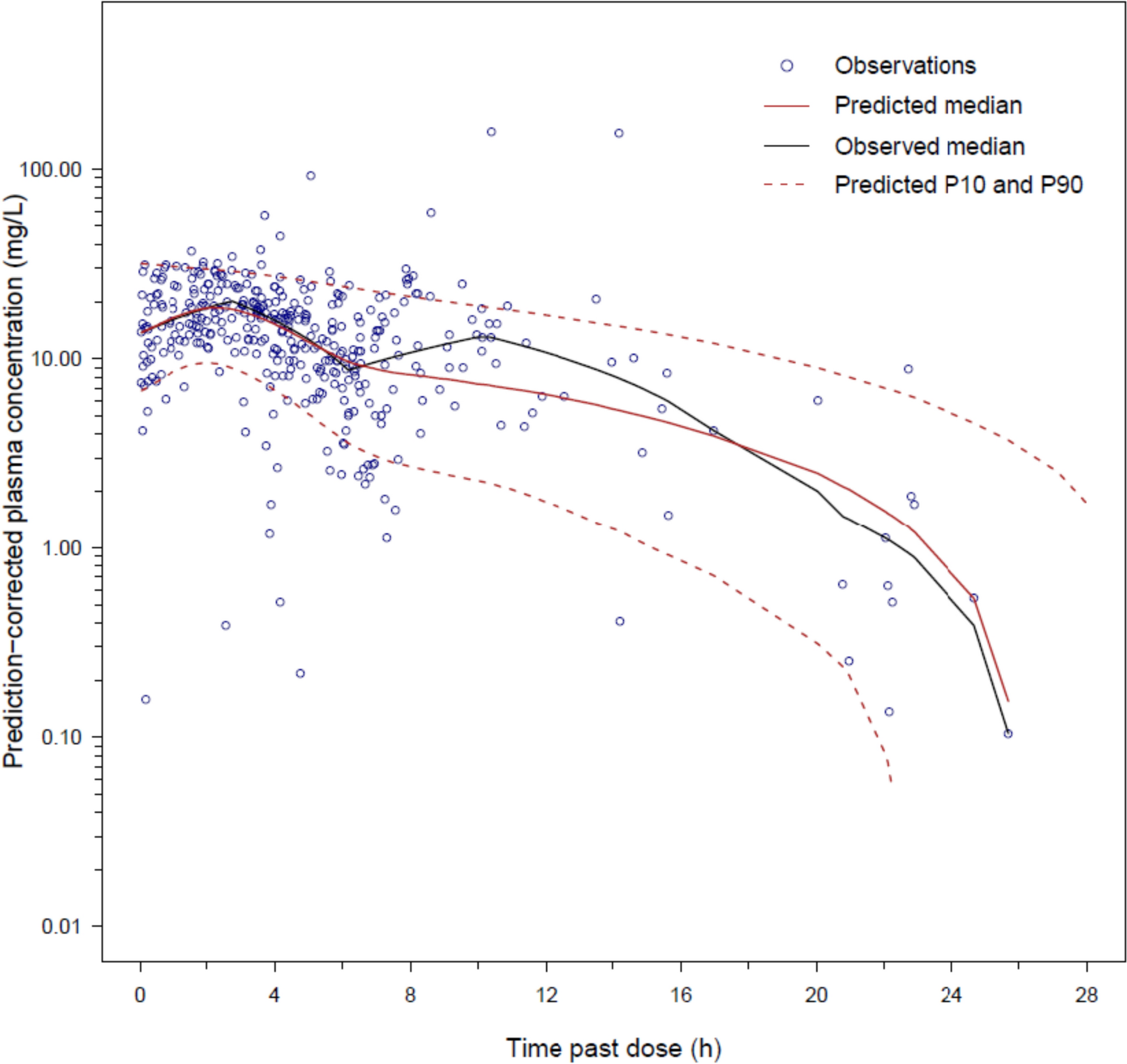
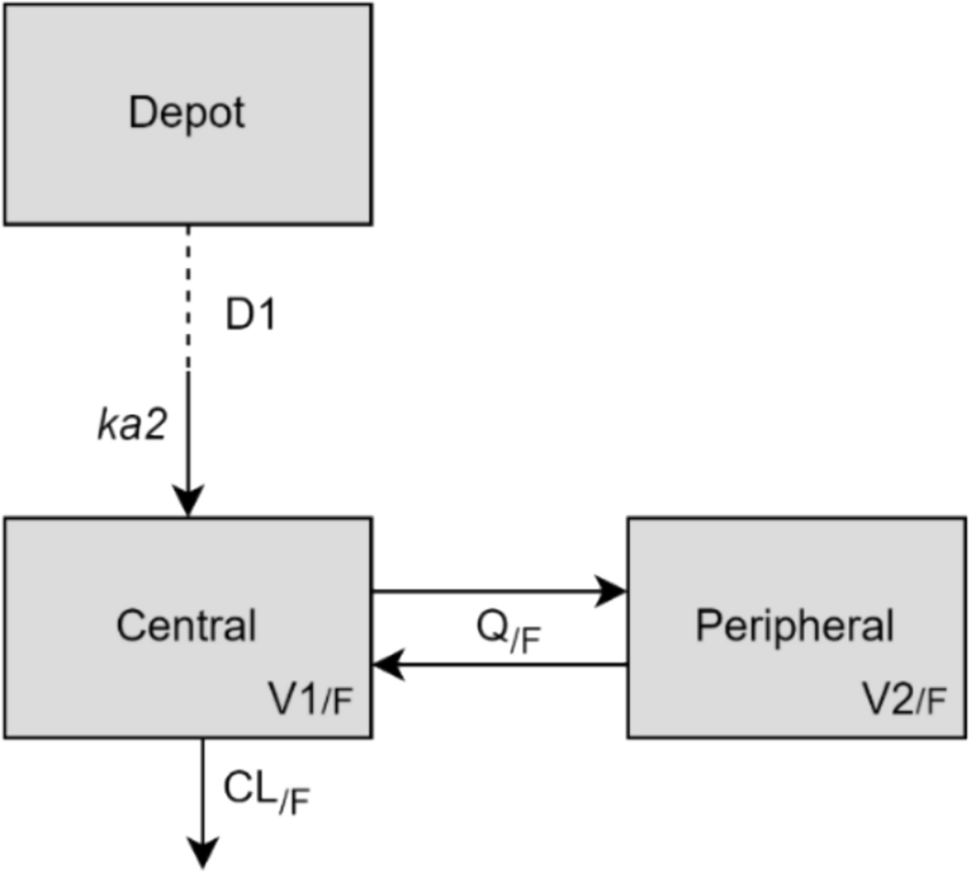
The developed two-compartment population model with linear elimination displayed the same structure as identified in previous population analyses of CPT, including an extensive study covering 21 phase I–III trials [10, 17, 27,28,29]. A different model describing CPT PK solely in healthy volunteers comprised three compartments, potentially supported by q12h dosing and longer periods of rich sampling (12 h) for all subjects [11]. Complete and fast in vivo CPT-F-to-CPT conversion has also been identified by studies with available measurements of both entities [10, 11, 17]. Linear elimination of CPT corresponded to another study in healthy volunteers assessing CPT PK after single-dose CPT-F (600 mg) [11]. Van Wart et al. identified parallel linear and Michaelis–Menten clearance of CPT, although they investigated a broad dose range of 50–2000 mg over a longer observation period (14 days). The study found adequate performance of a linear elimination model for CPT-F doses up to 1000 mg, which is in concordance with our study [10]. The PK parameter estimates were in the range of previous population PK analyses involving healthy volunteers (CL 10.9 L/h vs. 10.7 L/h for CLCR_median = 120 mL/min/1.73 m2 and agemedian = 28 years [17], 11.9 L/h for CLCR_median = 145 mL/min [11]; Vtotal 23.1 L vs. 19.0 L [17], 24.9 L for TBWmedian = 74.5 kg [11]). The interindividual variability associated with clearance was 15.6% and was in line with other studies including healthy volunteers (16.4% [11], 18.4% [30]). Potential sources of variability include renal excretion, factors influencing saturable elimination, or other covariates. In contrast to previous scientific evidence, yet not surprisingly, no significant impact of CLCR on CL was identified in the homogeneous, small population of healthy individuals, who displayed a limited range of unimpaired renal function (CLCR_C/G = 93.2–165 mL/min) [11, 12, 17].
Some limitations should be acknowledged with regard to the present investigation. First, our analysis exclusively considered healthy volunteers without altered pathophysiologic conditions and its results might not necessarily be transferable to infected patients with comorbidities, as suggested by a previous population PK analysis on CPT in patients with CAP, cSSTI and/or renal impairment versus healthy volunteers [17]. Highly variable exposure and faster drug elimination have been shown in infected patients, particularly in severely ill patients and those with augmented renal clearance, implying likely lower target attainment rates than in healthy volunteers [10, 31]. Thus, the dosing regimens required to attain specific PK/PD targets might differ between healthy volunteers and severely ill patients. Next, the small size and homogeneity of the healthy population with rather narrow ranges of clinical characteristics prevented a systematic covariate analysis, i.e. an investigation of the impact of patient factors such as renal function on ceftaroline PK and exposure. However, previous evidence implied only a minimal impact of body size and renal function on CPT target attainment in healthy volunteers [11]. Furthermore, the main purpose of our study was to identify trends in ƒT>MIC and target attainment with respect to different strategies of dosing intensification and bacterial susceptibility rather than causes of PK variability. Our investigation focused on three dosing components combined in the approved intensified dosing regimen [2]. Future exploration of continuous infusion seems relevant given its increasingly widespread use for β-lactams. To optimally and individually balance the interplay between infusion duration, dosing interval and daily dose in future studies, software tools enabling model-informed precision dosing represent a highly promising approach [32]. These tools consider a patient’s demographic and clinical characteristics, dosing history and, if available, measurement of the antibiotic concentration in blood (i.e. therapeutic drug monitoring sample) and allow the selection of an individualised dosing regimen aimed to meet a specific target.
The selection of a dosing regimen in clinical practice also depends on practicability. One vial of Zinforo® 600 mg powder for concentrate for solution for infusion contains 600 mg CPT-F [2]. Hence, two or three vials are required for the approved standard and intensified dosing regimen (and their equivalent with 1 and 2 h infusions), respectively. If 900 mg was used twice daily, four vials would be required to comply with ceftaroline stability (12 h at 2–8°C and 6 h at 25°C [2]); thus, the dosing regimen of 900 mg q12h appears to be the least cost-effective treatment option.




Comments (0)