
Remember me
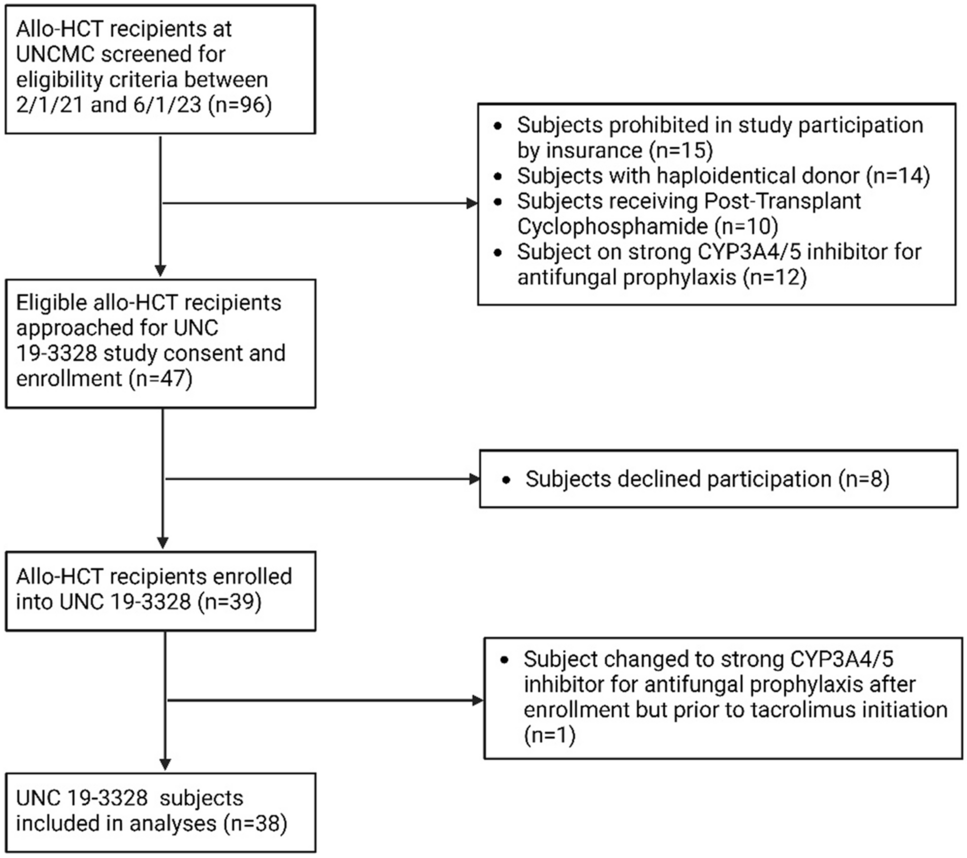
A total of 1126 articles were identified. After removing duplicates, 589 relevant studies were screened. Finally, 59 were assessed for title and abstract review, and 47 of them were included in the review (22 for micafungin, 13 for caspofungin, 9 for anidulafungin, and 3 for rezafungin) (Fig. 1).
Fig. 1
Flow chart of the article selection process
For the articles included the year of publication ranges across approximately 19 years (from 2004 to the end of 2023).
3.1.1 MicafunginMicafungin was the antifungal agent for which most models have been described (n = 22). The years of study included from 1998 to 2016. A total of 17 studies were conducted on adults and 5 on the pediatric population, one of which combined adults and pediatric patients. Nonlinear mixed‐effects modeling was the most widely used approach for describing micafungin PopPK models, with NONMEM being the most statistical modeling software used in 10 of the 22 models described (45.5%). The nonparametric adaptive grid (NPAG) algorithm for Pmetrics software was used in 8 out of 22 models (36.4%). Micafungin popPK was best described by a two-compartment approach (2-CMT) in 18 models and by a three-compartment approach (3-CMT) in 3 models. The study of Jullien et al. [34] had the largest population: 100 adults with 436 plasma concentrations, and the study of Hope et al. [24] had the largest pediatric population: 1919 samples in 229 patients. The percentage of males was higher than females in most studies. SCr levels were missing in some studies, especially in studies that included pediatric patients. Patients that were critically ill were the most widely studied population, with 12 of the 17 studies conducted on adults. The doses in adults ranged from 12.5 to 300 mg daily, with the dose of 100 mg/day being the most commonly used. In pediatrics, the doses ranged from 0.5 to 15 mg/kg/day. Treatment intention included prophylaxis, suspected and proven fungal infections.
The PD parameter most widely reported for assessing the drug exposure–efficacy relationship for micafungin, was the area under the concentration–time curve/MIC ratio (AUC0–24/MIC). The target most frequently reported for non-Candida parapsilosis spp varied between > 3000 and > 5000. However, the target AUC0–24/MIC > 285 for C. parapsilosis seems to be common in most studies. Some studies, such as Gastine et al. [30] and Zhong et al. [35] have suggested different targets depending on the specific Candida species.
3.1.2 CaspofunginA total of 13 models were described for caspofungin, 10 in adults and 3 in pediatrics. The studies were conducted between 1997 and 2021. NONMEM was the statistical modeling software most commonly used in 8 of the 13 models described (61.5%). Caspofungin popPK was best described using a 2-CMT approach in 11 models (84.6%). The study by Wu et al. [36] had the largest adult population with 58 patients (414 samples). In pediatrics, Yang et al. [37] included 48 patients with a total of 159 samples. Six studies [14, 15, 37,38,39,40] were conducted on the critically ill population including adults and children, and five on transplant recipients’ patients [28, 32, 36, 41, 42]. An LD of 70 mg followed by 50 or 70 mg/day according to body weight was the most common regimen, although in the study of Würthwein G. et al. [43], it was used up to 200 mg/day. The most used PD parameter to evaluate the correlation between drug exposure and efficacy was the AUC0–24/MIC ratio. According to Pressiat C. et al. for the fungicidal effect, an AUC0–24/MIC > 865 for C. albicans; > 450 for C. glabrata; > 1185 for C. parapsilosis were most widely reported, which corresponds to a free drug target of fAUC0–24/MIC > 25.9 for C. albicans; > 13.5 for C. glabrata; > 35.5 for C. parapsilosis. [28]. Only one study evaluated the PD target in Aspergillus spp. infections, reporting a target of Cmax/minimal effective concentration (MEC) of 10–20.
3.1.3 AnidulafunginA total of nine models were described for anidulafungin for adults. The period over which the studies were conducted has not been reported in most of them. The statistical modeling software most commonly used was NONMEM, in four of the nine models developed (44.4%). Anidulafungin popPK was best described using a 2-CMT approach in eight of the nine models described (88.9%). Patients that were critically ill were again the most commonly studied population, in five of the nine studies included [18, 22, 27, 44, 45]. A LD of 200 mg followed by 100 mg/day was the most common regimen, although in some studies a lower MD of 50 mg/day was used [46, 47]. Different PD parameters to evaluate the correlation between drug exposure and efficacy have been described, such as AUC0–24/MIC with a suggested but not clear threshold of 40 mg × h/L [47]; fAUC0–24/MIC > 20.6 for C. albicans, > 7.0 for C. glabrata; > 7.6 for C. parapsilosis in the study of Luque et al. [18] and Kapralos et al. [22] or AUC0–τ ≥ 82 h × mg/L for C. glabrata reported by Hall et al. [48].
3.1.4 RezafunginThe population PK of rezafungin has only been described in three studies, as this echinocandin has recently been marketed. The popPK models developed are more complex than the other three echinocandins; 4-compartment (4–CMT) and 3-compartment models (3–CMT) have been used. Doses vary widely, including single- and multiple-dose studies, ranging from 50 to 1400 mg, although the regular dose is LD 400 mg and MD 200 mg/weekly. The PD target has not been clearly defined for humans in the popPK studies conducted.
Table 1 summarizes the characteristics of the population pharmacokinetic studies included in the review. The data for the variability of each popPK model as well as the antifungal dosing recommendation of the included studies are summarized in Supplementary Table 1.
Table 1 Characteristics of the population pharmacokinetic studies included in the review3.2 Population Pharmacokinetic Analysis3.2.1 MicafunginAmong the 17 studies described for micafungin in adults, CL estimates ranged from 0.69 to 1.56 L/h for the 2-CMT models and 1.09 to 1.61 L/h for the 3-CMT models. The Vc estimates ranged from 8.84 to 17.6 L, the Vp ranged from 2.77 to 12.6 L for the 2-CMT models, and the Vc from 5.85 to 12.85 L for the 3-CMT models. The Vp (3.86 L) and Vpe (4.82 L) were only reported in the study of Garbez et al. [31] for the 3-CMT models.
The frequency of covariates included in the popPK model ranged from none to three for CL. Weight total (WT) was the most frequently reported significant predictor of micafungin CL, especially in pediatric patients and was included in the equations developed. In other models, SOFA, albumin, bilirubin, transaminases (ALT and AST), platelet count, body surface area (BSA), and fat free mass (FFM) have been reported to influence CL. For Vd, the developed equations were simpler; in seven models, no covariates were found, and in other 5 [20, 34, 54, 55, 60] WT was used as a significant predictor. In other models, the FFM [31] and the lean body mass corrected (LBMc) were included [56].
3.2.2 CaspofunginIn the ten models developed for caspofungin in adults, the CL estimates ranged from 0.21 to 0.70 L/h for the 2-CMT models; only one 3-CMT [40] was developed for adults with a predicted CL of 0.78 L/h. The CL in pediatric patients cannot be compared because they are expressed in different units. The Vc estimates ranged from 2.21 to 18.6 L and the Vp from 2.87 to 49.20 L for the 2-CMT models, and for the 3-CMT models, the Vc was 9.36 and Vp and Vpe 4.87 L and 4.69 L, respectively.
The frequency of covariates included in the popPK model ranged from none to two for CL. Six models [15, 28, 29, 38, 39, 41] did not find any covariate to influence CL; WT was only reported in two popPK models [14, 43]; FFM in one [40], and BSA in two pediatric models [32, 37]. The covariates most frequently described to influence the Vd for caspofungin popPK models were WT in four of ten adult models [14, 15, 35, 41], FFM in one model [40], and BSA in two pediatric models [32, 37]. Five models did not include any covariates to estimate the Vd [28, 29, 36, 39, 41].
3.2.3 AnidulafunginAmong the nine popPK models described for anidulafungin in adults, CL estimates ranged from 0.78 to 1.05 L/h for the 2-CMT models. Only one 3-CMT was described for adults with a mean CL of 1.00 L/h [21]. The Vc estimates ranged from 0.17 to 29.48 L and the Vp from 14.42 to 48.70 L for the 2-CMT models and for the 3-CMT model, the Vc, Vp2, and Vp3 were 16.60 L for all of them.
The covariates included in the anidulafungin popPK models for estimating the CL ranged from one to three. The WT was included in four models [18, 21, 44, 46], in one model FFM was included [27] and in another one, the lean body weight (LBW) [48]. The covariate most frequently described to influence the Vd was WT [21, 46, 47]. Other reported covariates were SOFA, Body mass index (BMI), LBW, and LBMc.
3.2.4 RezafunginOnly three popPK models have been described for rezafungin. The CL estimates ranged from 0.19 to 0.33 L/h and the Vc from 8.94 to 17.70 L for the 3-CMT and 4-CMT models developed. The covariates affecting the CL and the Vd differed between models. For CL, the BSA, disease state, WT, albumin, and sex were reported, while for Vd, the BSA, disease state, WT, infection, and albumin were included in the different models.
Table 2 summarizes the popPK model equations and mean values of the PK parameters (CL and Vd).
Table 2 Population pharmacokinetic model equations and mean values of the pharmacokinetic parameters3.3 Special Populations3.3.1 Critically ill patientsThe population of patients that are critically ill has been deeply studied in population PK studies for echinocandins. For micafungin, different popPK models have been developed. These models combined with an optimal sampling scheme, rapid identification of the Candida species and accurate susceptibility testing (MIC) provide an opportunity to achieve quick optimization of micafungin exposure and may guide early dose decision making [56]. The covariates included estimating the CL and Vd differed between models. WT has been mostly described but also SOFA, albumin, BSA, or ALT. To achieve the PK/PD targets, different approaches have been proposed in this population. In fungal peritonitis, the daily dose of 100 mg seems to be adequate to reach the PK/PD targets in plasma for Candida spp and, specifically, C. parapsilosis MICs of 0.008–0.016 and 0.125–0.25 mg/L, respectively [17]. In patients that are critically ill with severe burn injuries and patients with complicated intra-abdominal infections (IAI), 100 mg daily achieved the PK/PD targets in plasma for non-C. parapsilosis spp with MIC < 0.008 mg/L and C. parapsilosis with MIC < 0.064 mg/L, in both groups [52]. Nevertheless, the Vc was higher in patients with burns. In patients with sepsis and mechanical ventilation, 100 mg daily was associated with a very low probability of attaining the PK/PD target value in infections due to C. albicans or C. glabrata with MIC ≥ 0.015 mg/L, as well as in almost all cases of infection of C. parapsilosis. An increase in the dose should be considered in these cases [34]. In a cohort of Chinese patients that are septic, the recommended 100 mg daily had low clinical success for non-C. albicans infections; therefore, higher doses of at least 200 and 250 mg for MIC breakpoints of 0.032 and 0.064 mg/L for C. glabrata and C. tropicalis, respectively, should be considered. However, daily doses of 300 mg could not achieve MIC breakpoints of 0.125–0.25 mg/L for C. krusei and 1–2 mg/L for C. parapsilosis [35]. These results agree with Martial et al. [53] who stated that current micafungin dosing regimens are adequate to treat Candida infections with species up to 0.016 mg/L, but the dose should be increased to 200 mg in the case of MIC ≥ 0.032 mg/L. Kapralos et al. [23] proposed an alternative approach based on the use of a high LD. An LD of up to 300 mg for the treatment of IC in ICU patients may be needed, while an MD of up to 200 mg can be considered in empirical antifungal treatment.
For caspofungin, a weight-based dosing regimen supported by a popPK model has been proposed to reach the AUC target. An LD of 2 mg/kg, followed by 1.25 mg/kg as a MD, might be appropriate for achieving adequate exposure in ICU patients [38]. Martial et al. [53] suggested that the MD should not be reduced to 35 mg/day in ICU patients with moderate to severe hepatic dysfunction (classified as Child–Pugh B or C), contrary to what is indicated in the drug package insert. A MD of 70–100 mg in infections caused by pathogens with attenuated MIC > 0.125 mg/L, should be considered to achieve an optimal target attainment. For IAI treatment, due to the moderate penetration of caspofungin into the peritoneal cavity, in patients with FFM > 50 kg, an LD of 70 or 100 mg, with a MD of 70 mg, should be used to guarantee appropriate concentrations in the abdominal cavity for C. albicans and C. glabrata. While standard dosing regimens for patients with FFM < 50 kg for these species appear to be appropriate [40].
In the case of anidulafungin, a limited-sampling strategy may be useful for adequately estimating the exposure. The drug concentration can be adequately estimated from a single sample drawn 12 h after the start of the infusion either by linear regression or using a popPK model [27]. The PK of anidulafungin in ICU patients appeared to be comparable with the general population [44]. Another study reported that although drug exposure was comparable with that in healthy volunteers, elevated interindividual and significant interoccasion variability was found in patients that are critically ill [22]. In ICU patients with complicated IAI, the PK parameters were similar to healthy volunteers or other types of ICU patients. The standard dosage seems to be adequate in this population, although an increased Vd and a longer t1/2 were observed [45]. Luque et al. [18] recommended a higher dose of anidulafungin for the treatment of C. albicans or C. glabrata infections in patients that are critically ill with high TBWs > 150 kg to avoid potential clinical failures.
3.3.2 Renal Replacement TherapiesIn patients undergoing renal replacement, including continuous venovenous haemofiltration (CVVH), continuous venovenous hemodiafiltration (CVVHDF), continuous venovenous high cutoff membrane hemodialysis (CVVHD-HCO), and slow low-efficient daily dialysis (SLEDD), the data obtained for micafungin revealed no removal of it or need for dose adjustment for those patients, obtaining an optimal PK/PD coverage using the standard doses of this antifungal [16, 31, 49, 52]. Garbez et al. [16] recommended an LD of 150 mg to achieve the PK/PD target for less susceptible Candida species from the first day of therapy. For caspofungin, the two studies [
Comments (0)