
Remember me
The study was conducted in accordance with the protocol, International Council for Harmonisation (ICH) guidelines, applicable regulations and guidelines governing clinical study conduct, and ethical principles that have their origin in the Declaration of Helsinki. The protocol was approved by the institutional review board (IRB) or ethics committee, and all patients provided written informed consent before participation.
2.1 Study Design and ParticipantsThis was a phase 1, multicenter, multiple-dose, open-label, two-period, single-arm study designed to evaluate the impact of coadministration of multiple IV doses of risankizumab on the PK of CYP probe substrates using a cocktail approach in 20 adult patients with CD or UC (Clinicaltrials.gov: NCT04254783; Fig. 1).
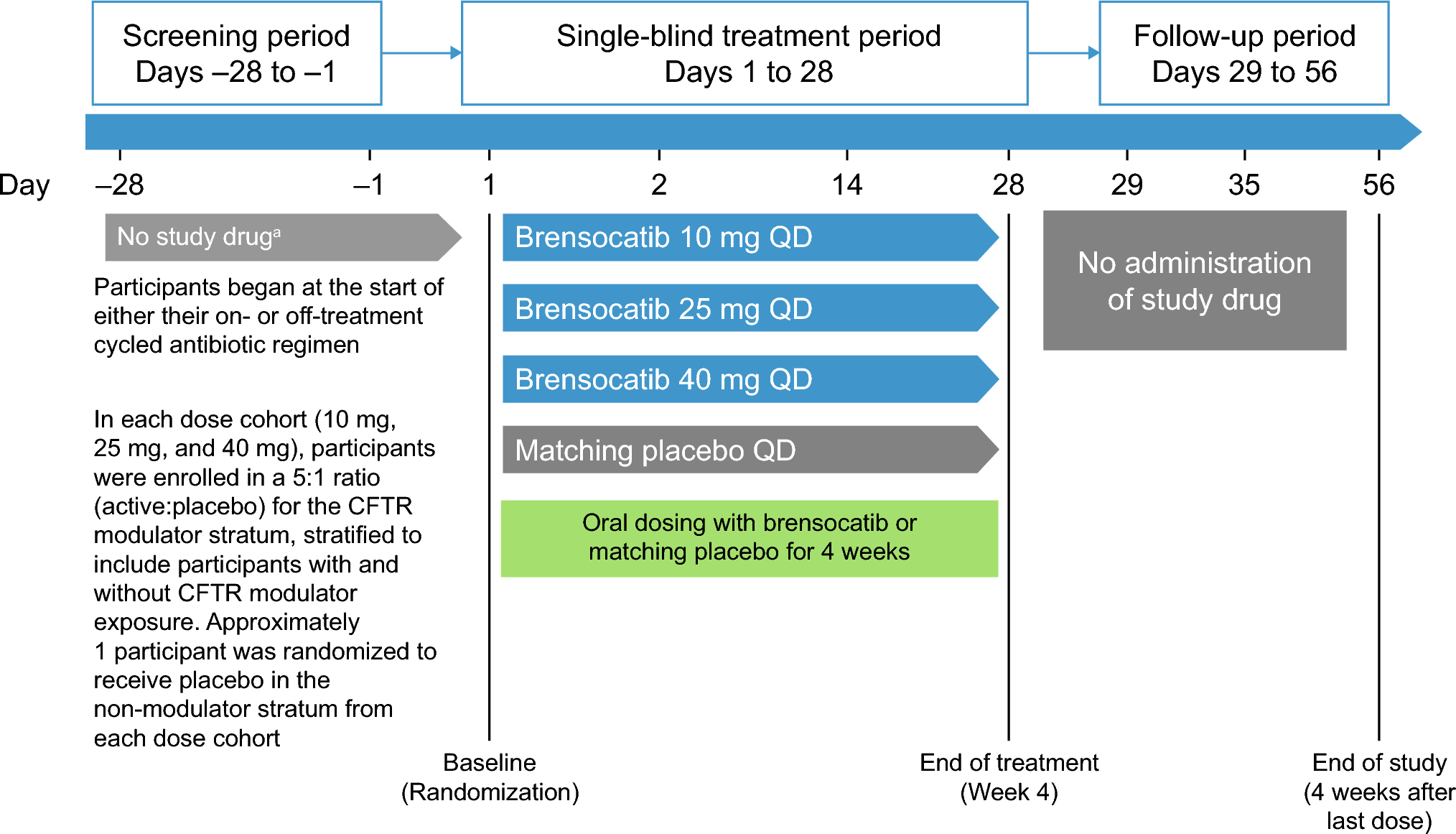
Fig. 1
Study design. AE adverse event, CD Crohn’s disease, COVID-19 coronavirus disease 2019, CYP cytochrome P450, IV intravenous, QxW every x weeks, SC subcutaneous, UC ulcerative colitis
In period 1, patients received a single oral dose of midazolam (2 mg; 1 mL of solution), caffeine (one 100-mg tablet or two 50-mg tablets), warfarin (one 10-mg tablet or two 5-mg tablets), vitamin K (two 5-mg tablets or 10-mg solution), omeprazole (one 20-mg capsule), and metoprolol (one 50-mg tablet) on day 1 under fasting conditions. Vitamin K was administered to these patients as a part of the cocktail to counteract the anticoagulant effect of warfarin, given CD and UC patients face a higher risk of bleeding. All study drugs in the CYP cocktail were taken with approximately 240 mL of water after a minimum 10-h fast and approximately 4 h before lunch. In period 2, patients received IV infusions of 1800 mg risankizumab over 3 h on days 1, 29, and 57 under non-fasting or fasting conditions, and a single oral dose of midazolam, caffeine, warfarin, vitamin K, omeprazole, and metoprolol on day 64 under fasting conditions. A minimum washout interval of 7 days separated the doses of CYP probe substrates in period 1 and the first dose of risankizumab in period 2. Optional subcutaneous (SC) doses to initiate maintenance treatment after period 2 were provided to patients who wished to continue risankizumab for the long-term treatment of their disease. After completion of period 2, patients could opt in to continue treatment with risankizumab maintenance therapy until they were transitioned to commercially available risankizumab or to an ongoing extension trial. To allow patients sufficient time to transition and to provide uninterrupted treatment to patients in the meanwhile, the study design included two optional visits for maintenance SC dosing.
Men and women with moderately to severely active CD or UC between 18 and 80 years of age, who had a body weight between ≥ 50.0 and ≤ 148.0 kg at screening and agreed to contraception requirements were eligible to participate. Participants were required to have a confirmed diagnosis of CD (average daily stool frequency ≥ 4 and/or average daily abdominal pain score ≥ 2, and a Simple Endoscopic Score-CD of ≥ 6 [or ≥ 4 for isolated ileal disease]) for at least 3 months prior to baseline or UC (adapted Mayo score of 5–9 and endoscopic subscore ≥ 2 confirmed by a central reader), and demonstrated intolerance or inadequate response to one or more of the following categories of drugs: aminosalicylates, oral locally acting steroids, systemic steroids, immunomodulators, and/or approved biologic therapies/small molecules. Patients could receive a therapeutic dose of disease-related antibiotics and/or oral or topical 5-aminosalicylic acid compounds provided that the dose was stable for 2 weeks prior to day −1; azathioprine (AZA), 6-mercaptopurine (6-MP), or methotrexate (MTX) provided that the current course was ≥ 42 days prior to day −1 and was stable for ≥ 28 days prior to day −1; and oral corticosteroid therapy provided the current course was ≥ 14 days prior to day −1 and was stable for ≥ 7 days prior to day −1. Patients were not eligible if they received any live bacterial or viral vaccination within 28 days prior to screening; received cyclosporine, tacrolimus, or mycophenolate mofetil; or received fecal microbial transplantation within 28 days prior to day −1. Patients were not eligible if they were treated with any investigational drug within 30 days or five half-lives of the drug (whichever is longer) prior to the first dose of study drug and if they had used any known inducers or inhibitors of CYP1A2, CYP2C9, CYP2C19, CYP2D6, or CYP3A4, including dietary supplements or herbal products containing St. John’s wort or other known CYP inhibitors or inducers within 1 month or five half-lives, whichever was greater, before administration of the first cocktail probe. No consumption of grapefruit products, Seville oranges, starfruit products, quinine/tonic water, dietary/herbal supplements, and inhibitors of P-glycoprotein, breast cancer resistance protein, and organic anion-transporting polypeptide 1B1/1B3 transporters was allowed within 14 days or five half-lives before administration of the cocktail. Patients were required to agree to not use any of the above products until after the last PK sample was collected, 7 days after the last intake of the probe cocktail. Intake of caffeine was controlled on the days of cocktail administration.
Patients were confined to the study site and supervised for approximately 20 days total during the following intervals: (1) Confinement in period 1 began on day −2 or day −1 (up to 2 days prior to study drug dosing) and ended after the collection of the 168-h blood samples and completion of scheduled study procedures on day 1 of period 2. (2) Confinement in period 2 began on day 62 or day 63 and ended after the collection of the 168-h blood samples and completion of scheduled study procedures on day 71 of period 2. Patients were allowed to leave the study site between periods 1 and 2. On all other study days, the study was performed on an outpatient basis, during which the patients visited the study site to complete scheduled study procedures.
2.2 Pharmacokinetic Sampling and Bioanalytical MethodsSerial blood samples for determination of CYP probe substrate and metabolite plasma concentrations were collected by venipuncture into sodium heparin-containing tubes prior to dosing (0 h) and for up to 24 h after dosing for midazolam, omeprazole, and 5-hydroxy-omeprazole (5-OH-omeprazole; metabolite formed by CYP2C19) on period 1 day 1 and period 2 day 64; up to 48 h after dosing for caffeine and metoprolol on period 1 day 1 and period 2 day 64; and up to 168 h after dosing for warfarin on period 1 day 1 and period 2 day 64. Plasma concentrations of midazolam, caffeine, S-warfarin, R-warfarin, omeprazole, 5-OH-omeprazole, and metoprolol were determined using validated assays developed by PPD Laboratories (Middleton, WI, USA). Briefly, the plasma samples were first combined with internal standards for each of the analytes, then isolated, extracted, and reconstituted before being analyzed using either high-pressure liquid chromatography‐tandem mass spectrometry (HPLC‐MS/MS) or ultra-performance liquid chromatography (UPLC) with MS/MS detection. The lower limit of quantification (LLOQ) was 0.100 ng/mL, 25 ng/mL, 5 ng/mL, 1.0 ng/mL, and 0.2 ng/mL for midazolam, caffeine, S- and R-warfarin, omeprazole and 5-OH-omeprazole, and metoprolol, respectively. The bias values across the assays were within ± 5%, and the percentage coefficients of variation (%CV; as a measure for precision) across the assays were < 11%. No interference for simultaneous testing of these analytes was observed.
Note that both S- and R-warfarin were evaluated in the study to provide a comprehensive assessment of potential DDIs. Warfarin was selected for evaluation as a sensitive CYP2C9 probe, and given the S-warfarin enantiomer is primarily metabolized by CYP2C9, its evaluation was essential for this DDI study. R-warfarin, metabolized by CYP1A2, CYP3A4, and CYP2C19, was included to thoroughly investigate risankizumab’s potential impact on these enzymes. While R-warfarin's evaluation was not critical for CYP2C9-mediated interactions, its inclusion aligned with the broader study objective of assessing interactions involving multiple CYP enzymes.
Blood samples for risankizumab serum concentrations were collected in period 2 prior to dosing on days 1, 29, and 57, and on days 64, 71, and 169. Blood samples for the detection of risankizumab anti-drug antibody (ADA) were collected in period 2 prior to dosing on days 1, 29 and 57, and on day 169. Serum concentrations of risankizumab were determined using a validated bridging electrochemiluminescence immunoassay. The LLOQ for risankizumab was established at 4.34 ng/mL. Samples quantified below the LLOQ were reported as zero. The presence of ADA was determined by using a validated titer-based bridging electrochemiluminescence immunoassay via a tiered approach (screening, confirmation, and titration), with a drug tolerance of 100 ng/mL positive control antibody being detectable in the presence of 100 or 102 μg/mL risankizumab. Patients were defined as treatment-emergent ADA positive as follows: (1) when they were ADA negative or missing assessment at pre-dose baseline and became ADA positive at one or more time points after baseline; or (2) when they were ADA positive at baseline and exhibited a fourfold or greater increase in titer values relative to baseline.
2.3 Pharmacogenetic Analysis of Polymorphic Cytochrome P450 EnzymesOne 4-mL whole-blood sample was collected from each patient for pharmacogenetic analyses of polymorphisms in the genes encoding CYP2C9, CYP2C19, and CYP2D6. DNA was isolated from whole blood using Qiagen reagent kits (Qiagen Inc., Valencia, CA) applied to an AutoGenprep 3000 automated DNA extraction instrument. DNA samples were processed following the procedures described in the PharmacoScan™ Assay 24-Array Format (Applied Biosystems, Waltham, MA), ThermoFisher Catalog number 903010TS. CYP2D6 × 2 and s5 alleles were also measured using polymerase chain reaction (PCR) and gel electrophoresis [16, 17]. Blood samples were genotyped for the presence of the following alleles: CYP2C9, *2, *3, *5; CYP2D6, *2, *3, *4, *5, *6, *7, *9, *29, *35, *41; and CYP2C19, *2, *3, *4, *8, *10, *12, *17. Genotypes and phenotypes were determined using the Axion Analysis Suite (Applied Biosystems, Waltham, MA) version 4.0.3.3 for array type PharmacoScan_24F.R8 with Best Practice workflow and confirmed using the functionality allele provided in the CPIC website. References were also made with websites PharmGKB [18] and Clinical Pharmacogenetics Implementation Consortium (CPIC) [19].
2.4 Pharmacokinetic and Statistical AnalysesPlasma concentrations and PK parameter values (maximum plasma concentration [Cmax], time to maximum plasma concentration [Tmax], area under the concentration–time curve from time 0 to time t [AUCt], area under the concentration–time curve from time 0 to infinity [AUCinf], terminal t½) for each of the CYP probe substrates and their metabolites (if applicable) were calculated for each participant, and summary statistics were tabulated for each sampling time using noncompartmental methods in SAS® version 9.4 (SAS Institute, Inc., Cary, NC, USA). The ratio of metabolite area under the curve (AUC) to parent drug AUC was also tabulated for omeprazole.
To assess the effect of risankizumab on each of the CYP probe drugs, the two one-sided tests procedure was performed on log-transformed AUCinf, AUCt and Cmax for each of the CYP probe drugs and 5-OH-omeprazole (metabolite of omeprazole), and on log-transformed AUCt and AUCinf of metabolite-to-parent drug ratios for 5-OH-omeprazole/omeprazole, via 90% confidence intervals (CIs) for the ratio of regimen central values.
Point estimates of the ratios of the geometric means (test/reference) for the primary endpoints of CYP probes during co-administration with risankizumab and the additional endpoints AUCt metabolite/AUCt parent (RAUCt) and AUCinf metabolite/AUCinf parent (RAUCinf) for omeprazole (5-OH-omeprazole/omeprazole), and their two-sided 90% CIs, were provided.
Additionally, sensitivity analyses were performed for the CYP2C9 and CYP2D6 substrates to assess the effect of risankizumab on CYP substrates after excluding patients with poor metabolizer phenotypes. This was accomplished by re-running the primary statistical analysis on the log-transformed Cmax, AUCt, and AUCinf after excluding patients with the poor metabolizer phenotype.
2.5 Safety AssessmentsSafety was evaluated during confinement and at each study visit through physical examination, vital signs, clinical laboratory tests, electrocardiogram (ECG) assessments, and adverse event (AE) monitoring.
Comments (0)