
Remember me

Multiple compounds are currently under investigation at different stages of development to fill the remaining gaps in the first and the second-line (or later) of treatment in the rapidly evolving treatment paradigm for R/M CC. Building on the success of pembrolizumab in the first-line setting, the identification of alternative therapeutic options in the subsequent lines became a new clinical unmet need. In the precision oncology era, tailored treatments are developed with the purpose of increasing the efficacy of anticancer drugs by minimizing at the same time their systemic distribution and targeting specific molecular markers, selectively expressed by cancer cells, thus avoiding off-target effects. In this context, ADCs represent a new promising strategy to address this issue. Additionally, ICIs combination therapies, including dual checkpoint inhibition and multi-drug approaches to complement ICIs using TME-immunomodulating agents, are currently being evaluated to address the emerging immune checkpoint blockade resistance issue, which will be the next unmet clinical need arising from the current extensive use of immunotherapy in earlier settings.
Moving forward, since different trials are currently investigating the effect of immunotherapy in addition to chemoradiation in the management of locally advanced CC, ICIs may move into earlier stages of therapy. Hence, there might be the need for novel approaches in the next future even in the upfront setting. In this scenario, ICIs combination treatments may represent a promising approach to replace chemotherapy or as an alternative option in patients who do not tolerate it. Besides, alternative agents to ICIs in the first-line setting are under investigation in several clinical trials to enhance the efficacy of chemotherapy.
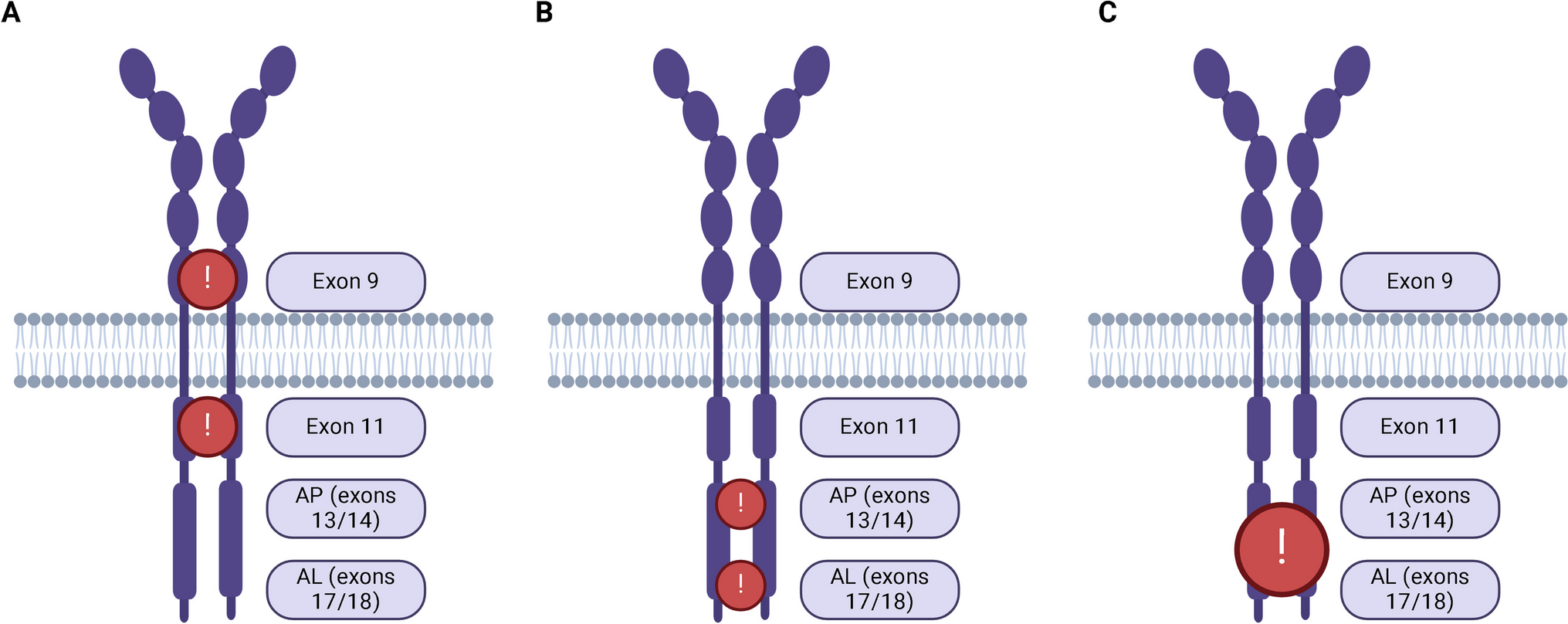
ADCs: Effective Agents Alternative to ICIs in the Post-platinum Setting and Promising Drugs to Complement ICIs and ChemotherapyWith their complex structure, composed of three main components, ADCs target specific antigens expressed by tumor surfaces through the interaction of the monoclonal antibody (mAb) with the specific target, which covalently binds a cytotoxic agent via a chemical linker. Moreover, beyond the cytotoxic effect on the targeted cell, driven by the release of the payload in the lysosomes with the consequent cell apoptosis or death via targeting DNA or microtubules, ADCs are able to provoke a bystander effect on neighborhoods cells, and to alter the tumor microenvironment (TME), further enhancing their antitumor effect [27]. The evidence of a high expression of tissue factor (TF) on CC surfaces, along with its critical role in promoting tumor growth and progression, and angiogenesis within the TME [28], led to the development of a new ADC, tisotumab-vedotin (TV), which binds TF through a fully humanized mAb linked via a cleavable mc-VC-PABC to the cytotoxic payload monomethyl auristatin E (MMAE), an antimitotic agent which induces G2/M cell cycle arrest, finally leading to cell death [29]. Adverse events (AEs) of special interest (AESI) are manageable, represented by ocular toxicity, neuropathy, and bleeding. Conjunctivitis (26%), dry eye (23%), and keratitis (11%) are the most common treatment-related ocular events, the majority of those managed with corticosteroids, vasoconstrictors eye drops, and recovered within 30 days after the last dose. Besides, Grade < 3 bleedings frequently occur, including the most common epistaxis (30%), followed by vaginal hemorrhage (7%), and hematuria (3%), more likely without any intervention required. Finally, neuropathy (peripheral, sensory, or sensorimotor) is generally short-term (time to resolution: 0.6 months) and Grade < 3 [30•].
ADCs MonotherapyThe first-in-human, phase I/II, innovaTV 201 study showed promising antitumor activity of TV among patients with refractory solid tumors (ORR: 15.6%, 95% CI 10.2 to 22.5%; mDoR: 5.7 months, 95% CI 3.0 to 9.5 months) [30•], and encouraging results were observed in the previously treated, CC cohort (ORR: 24%, mDoR: 4.2 months, and 6-month PFS: 29%) [31]. ORR of 24% was further confirmed in the phase II InnovaTV 204//GOG-3023/ENGOT-cx6, specifically designed to investigate the antitumor activity in pre-treated, R/M CC patients, demonstrating even better results in terms of mDoR (8.3 months, 95% CI 4.2 to NR) and mPFS (4.2 months, 95% CI 3.0 to 4.4 months) [32••]. Similar results were also observed in the InnovaTV 206 study, showing an ORR of 29.4% (95% CI, 10.3% to 56.0%), mDoR of 7.1 months (3.1 months to NR), mPFS of 3.1 months (95% CI, 1.2 to 7.1 months), and mOS of 11.4 months (95% CI, 6.2 months to NR) in a Chinese patient population [33] (Table 1). These data led to the first FDA-approval of ADCs in the CC treatment landscape in late 2021, giving a valid alternative therapeutic option to pembrolizumab, especially for PD-L1-positive, CC patients previously treated in the first-line setting with pembrolizumab in addition to platinum-based chemotherapy with or without bevacizumab (Fig. 1). The randomized, phase III, ENGOT CX12/GOG-3057/INNOVATV 301 trial is ongoing to finally confirm the efficacy of TV compared to standard chemotherapy in previously treated R/M CC patients (NCT04697628, Table 2).
ADCs: Combination ApproachesGiven the immunomodulatory properties of ADCs and the effectiveness of TV in CC patients regardless the PD-L1 status, this novel therapeutic approach is under investigation in several clinical trials in combination with other anticancer-agents (Fig. 1).
In the first-line setting, TV demonstrated to be a valid alternative option to ICIs in order to complement chemotherapy. The second part of the phase Ib/II ENGOT-cx8/GOG-3024/innovaTV 205 clinical trial demonstrated promising antitumor activity with acceptable safety profile with the use of TV in combination with carboplatin in chemo naïve, R/M CC patients. Preliminary results showed an ORR of 55% (95% CI 36 to 72), which is higher than the historical RR (48%) observed with platinum-based chemotherapy given in combination with bevacizumab [14]. Besides, a mDoR of 5.6 months, and mPFS of 6.9 months at a median follow-up of 4.8 months were observed (Table 3), along with manageable toxicity (ocular events grade 1–2 and grade ≥ 3 in 55% and 3% of patients respectively), peripheral neuropathy (grade 1–2: 27%, grade ≥ 3: 12%) and bleeding events (grade 1–2: 48%, grade ≥ 3: 6%). [34]. Further, the above-cited immunogenic properties of TV, along with the proven ADCs ability to increase T lymphocyte infiltration and to induce dendritic cell maturation, and co-stimulatory molecules expression, gave the basis to explore the synergistic effect of TV in combination with immunotherapy [35, 36]. Indeed, the combination of TV and ICIs was tested both in the chemo-naïve setting and after the failure of the first-line treatment in different trials (Tables 1 and 3).
In the first-line setting, the combination of TV with pembrolizumab was investigated with the aim of replacing chemotherapy, showing an ORR of 41% (95% CI 24 to 59) and mPFS of 5.3 months (95% CI, 4.0 to 12.2) in a cohort of the ENGOT Cx8/GOG 3024/innovaTV-205 trial, thus confirming the synergistic activity of TV and pembrolizumab in the chemo naïve CC population, with manageable toxicity (alopecia: 61%, diarrhea: 55%, epistaxis: 49%, conjunctivitis: 46%, and nausea: 46%) [37]. Besides, TV is currently under investigation in a cohort of the phase Ib/II ENGOT-cx8/GOG-3024/innovaTV 205, even to test the addition of this agent to the quadruplet therapy studied in the KEYNOTE-826 study, which might be a promising strategy to complement chemotherapy in the first-line setting for R/M CC patients who are not eligible to pembrolizumab plus platinum-based chemotherapy because of CPS < 1 (Table 2) [38].
Finally, TV-pembrolizumab combination therapy was also investigated in the recurrent setting after the failure of the first-line treatment. Clinical benefit was observed in the previously treated cohort of R/M CC patients enrolled in the phase I/II ENGOT Cx8/GOG 3024/innovaTV-205 trial. Indeed, promising ORR was observed (ORR: 38%, 95% CI: 22 to 56), along with durable responses (mDoR: 13.8 months, 95% CI: 2.8 to NR), and encouraging survival rates (mPFS: 5.6, 95% CI: 2.7 to 13.7 months; mOS: NR, range 1.3–17.5 + months) after median 13 months of follow-up (Table 1) [34].
Combination Strategies to Overcome ICI Resistance: Dual Checkpoint Inhibition and Immunomodulatory Agents in Addition to ICIsA promising approach deeply investigated in the clinical setting to overcome resistance and broaden the efficacy of anti-PD-1 agents is the concomitant dual checkpoint inhibition, by concomitantly blocking two co-inhibitory pathways. The most reliable targets to achieve a synergistic effect with anti-PD-1 antibodies include the blockade of CTLA-4 and T cell immunoreceptor with immunoglobulin and ITIM domains (TIGIT) co-inhibitory signals. CTLA-4 and PD-1 are potent immune checkpoint cell surface receptors involved in the downregulation of T cell response to physiologically establish cell tolerance. However, their expression patterns are spatially and temporally distinct [39], thus suggesting a complementary activity of those two pathways in limiting autoreactivity. Based on this rationale, the dual inhibition of those pathways entered the clinical setting, demonstrating durable clinical activity among different cancer types. Concerning CC, durable clinical activities were observed especially in the PD-L1 negative population both in chemo naïve and previously pretreated R/M CC population.
Besides, the evidence of an immunomodulatory effect of anti-angiogenetic agents represented an attractive strategy to complement ICIs. Specifically, the aberrant nature of the cancer vessels, along with the production of pro-angiogenic factors by cancer cells, demonstrated to induce both physical and chemical barriers to the immune response, by inhibiting lymphocyte trafficking across endothelia and migration into tumor deposits due to the increase of interstitial pressure, and by the recruitment of immunosuppressive cells due to increased hypoxia within the TME [40,41,42]. On the other hand, the enhanced expression of coinhibitory factors of the immune response might contribute to anti-angiogenic drugs resistance [23, 43, 44]. Given this strong interplay between the two pathways, the combination of immune checkpoint blockade and tyrosine kinase inhibitors (TKI) targeting the VEGF signal pathway entered the clinic and has been evaluated as a treatment strategy to enhance responses to immunotherapy.
Dual Checkpoint InhibitionThe addition of dual checkpoint inhibition to standard chemotherapy with or without bevacizumab represents a promising strategy to cover the full spectrum of the R/M CC population, regardless of PD-L1 expression (Fig. 1). In this context, a bispecific antibody targeting PD-1/CTLA-4, cadonilimab (AK104), was tested in an open-label, phase II study, having enrolled patients in three different cohorts: cohorts A-15 and A-10 were the two cohorts investigating AK104 in combination with platinum-based chemotherapy at two different dosages (AK104 15 mg/kg and 10 mg/kg, respectively) and cohort B-10 was the third cohort investigating AK104 10 mg/kg in combination with platinum-based chemotherapy plus bevacizumab. Impressive results were shown, regardless of PD-L1 status. The secondary endpoint ORR was promising across all three cohorts: specifically, ORRs were 73.3%, 68.8%, and 92.3% in the A-10, A1-15, and B-10 cohorts respectively (Table 3) [45], thus warranting further investigation to evaluate the efficacy in a phase III ongoing trial (NCT04982237, Table 2). Concerning the safety profile, this combination was well tolerated, with the most common grade ≥ 3 treatment-related AEs (TRAEs) belonging to hematological toxicity (anemia: 15.6%, white blood cell count decreased: 11.1%, neutrophil count decreased: 8.9% and platelet count decreased: 8.9%), and grade ≥ 3 immune-related AEs (irAEs) occurring in 17.8% patients. Nonetheless, long-term safety follow-up is awaited.
Besides, the impressive effectiveness of immune checkpoint blockade, which has broken new ground in CC research, further prompts the investigation of immunotherapy in completely replacing chemotherapy as the upfront line of treatment for R/M CC patients (Fig. 1). The phase I/II CheckMate 358 study investigated nivolumab alone or in combination with ipilimumab as a chemotherapy-free regimen for the first-line treatment, showing manageable toxicity and durable tumor regression regardless of tumor PD-L1 expression in patients with R/M CC. With a minimum follow-up of 24 months, the primary endpoint ORR was encouraging either with nivolumab monotherapy (anti PD-1, ORR: 26%, 95% CI 9 to 51%) or in combination with the anti-CTLA-4 inhibitor, ipilimumab, given in two different regimens, namely nivolumab 3 mg/kg every 2 weeks + ipilimumab 1 mg/kg every 6 weeks (N3 + I1 arm, ORR: 39%, 95% CI 17 to 64%), nivolumab 1 mg/kg every 2 weeks + ipilimumab 3 mg/kg every three weeks × 4 cycles followed by nivolumab 240 mg every 2 weeks (N1 + I3 arm, ORR: 41%, 95% CI 29 to 53%), (Table 3). Durable responses were observed across all three arms, with durable responses observed even in the PD-L1 negative population. Notably, higher grade ⩾3 TRAEs (16% versus 5%) and discontinuation rates (24% versus 18%) were observed in arm N1 + I3 arm compared with arm N3 + I1 arm [46].
In addition to the promising role of dual checkpoint inhibition to extend the use of immunotherapy even in the PD-L1 negative, chemo naïve, CC population, this therapeutic strategy was also tested in previously treated R/M CC patients with the aim of overcoming anti-PD-1 resistance (Fig. 1). In the I/II CheckMate-358, the combination of nivolumab (anti-PD-1) and ipilimumab (anti-CTLA-4) was also tested in R/M CC after the failure of the first-line treatment, and regardless of PD-L1 status. Encouraging clinical activity (ORR: 26%, 95% CI 11 to 46 in the N3 + I1 arm; ORR: 35%, 95% CI 21 to 51 in the N1 + I3 arm), along with durable responses (mDoR: 21.1 months, 95% CI, 7.5 to NR in the N3 + I1 arm; mDoR: NR, 95% CI, 5.2 to NR in the N1 + I3 arm at a minimum follow-up of 24 months) were observed.
Similar results were found in a phase II study investigating the safety and efficacy of bastilimab (anti-PD-1) and zalifrelimab (anti-CTLA-4) combination therapy as second-line treatment, with reported ORR of 25.6% (95% CI, 18.8 to 33.9) and mDoR NR (95% CI, 9.7 to NR) after 21 months as a median follow-up (Table 1). The 12-month PFS and OS rates were 21.3% (95% CI, 14.1 to 29.4) and 53.3% (95% CI, 43.8 to 61.9), respectively, with a median PFS of 2.7 months (95% CI, 1.5 to 3.7), and a median OS of 12.8 months (95% CI, 8.8 to 17.6) [47]. Furthermore, this combination strategy was well tolerated, without any unexpected TREAs and with a rate of grade ≥ 3 TRAEs (20%) consistent with previous studies investigating the anti-PD-1/ anti-CTLA-4 combination strategy [47].
Accordingly, the randomized phase RaPiDS/GOG-3028 II study is further assessing the safety and efficacy of bastilimab, both alone and in combination with zalifrelimab, compared with standard chemotherapy in the second-line setting (NCT03894215, Table 2). Besides, promising clinical activity was further observed in the phase II clinical study, with the bispecific antibody AK104, targeting both PD-1 and CTLA-4. Observed ORR was 33% (95% CI, 23.9 to 43.1), and mDoR NR (95% CI, 0.95 to 16.43) at a median follow-up of 9.63 months (Table 1). In line with the previously mentioned trial, tumor response was not related to the PD-L1 status [48]. Moreover, based on results from the first part of a phase II study (CTR20202017) conducted in China, the combination of IBI310 (anti-CTLA-4) and sintilimab (anti-PD-1) received the Breakthrough Therapy Designation by the Center for Drug Evaluation of China’s National Medical Products Administration (NMPA). The combination is under study in phase II, in a randomized trial to compare the efficacy of sintilimab monotherapy to IBI310 (anti-CTLA-4) and sintilimab combination therapy (NCT04590599, Table 2).
Beyond CTLA-4 and PD-1, TIGIT is one of the other checkpoint inhibitory receptors, involved in limiting effector T cell survival and function. TIGIT is structurally and functionally different from CTLA-4 and PD-1, due to its ITIM domain, and because of the ability to further suppress the innate immune response [49]. Several trials are ongoing to investigate the efficacy of PD-1 and TIGIT dual inhibition (NCT04693234, NCT05007106, NCT04300647, Table 2). Preliminary data came from the phase I KEYVIBE-001 study, investigating the pembrolizumab (anti-PD-1)/vibostolimab (anti-TIGIT) combination therapy. In this study pembrolizumab was tested in combination with two different dosages of vibostolimab (200 mg versus 700 mg every3 weeks), demonstrating comparable antitumor activity and safety. After a median follow-up of 11.5 months, ORR of 15% and 23% were observed in the two cohorts (vibostolimab 200 mg versus 700 mg, respectively) and mDoR was not reached (NR, range 10 to 31 + months in the vibostolimab 200 mg cohort; NR, range 4 + to 35 + months in the vibostolimab 700 mg cohort), irrespective to PD-L1 status (Table 1), with evidence of grade ≥ 3 TRAEs in 18%-29% of patients [50]. The recommended phase 2 dose for vibostolimab (200 mg every 3 weeks) is currently under evaluation in combination with pembrolizumab in the phase II KEYVIBE-005 study to evaluate the efficacy both in PD-L1–positive (CPS ≥ 1) and PD-L1–negative CC patients (NCT05007106, Table 2).
ICIs in combination with TKIThe first reported study to evaluate the concurrent inhibition of immune checkpoint and angiogenetic pathways in previously treated R/M CC patients was the CLAP trial. In this single-arm, phase II study, the combination of the PD-1 inhibitor camrelizumab with the selectively VEGFR2 inhibitor apatinib demonstrated its clinical activity regardless of the expression of PD-L1. ORR was 55.6% (95% CI, 40.0% to 70.4%), mPFS 8.8 months (95% CI, 5.6 to NR) and after a median follow-up of 11.3 months, neither mDoR nor mOS were reached (mDoR: NR, 95% CI: 5.6 to NR; mOS: NR, 95% CI: 11.6 to NR) [51] (Table 1). Interestingly, an exploratory analysis of the trial aiming at identifying alternative biomarkers to PD-L1 to predict response found a correlation between favorable clinical outcomes and gene alterations in the PI3K/AKT pathway [52]. Based on those encouraging results, camrelizumab-apatinib is currently under study even in the first-line setting, in a randomized, phase 2 trial to assess the efficacy of this combination compared to platinum-based chemotherapy plus bevacizumab in patients with R/M CC patients (NCT04974944, Table 2).
Camrelizumab was further tested in combination with famitinib, a multikinase inhibitor with a broad spectrum of targets, including VEGFR2 and 3, platelet-derived growth factor receptor β (PDGFRβ), FMS-like tyrosine kinase-1/3 receptor, proto-oncogene tyrosine-protein kinase receptor, and the stem-cell factor receptor (Table 1). Efficacy analysis of the phase II single-arm trial showed ORR of 39.4% (95% CI, 22.9 to 57.9), and mPFS of 10.3 months (95% CI, 3.5 to NR). After a median follow-up lasting for 13.6 months, mDoR was NR (95% CI, 8.2 to NR), and the 12-month OS rate was 77.7% (95% CI: 58.9–88.7) [53]. Given this promising clinical activity, along with a manageable safety profile, a randomized, open-label, 3-arm phase 2 trial was developed and is currently ongoing to investigate the efficacy of this combination compared to standard chemotherapy (NCT04680988) in the same setting (Table 2).
Positive signals with the use of TKI to extend ICIs indication to a broad population, further came from the preliminary results of the ENGOT-GYN3/AGO/LIO study. In this trial, PD-1 inhibitor nivolumab was given in combination with lucitanib, a potent inhibitor of VEGFR1–3, PDGFRα/β, and fibroblast growth factor receptor (FGFR) 1–3. Data from stage 1 of the phase II CC cohort were recently reported, showing target lesion reductions even in CC in the PD-L1 negative population, with manageable toxicity (Table 1) [54].
Finally, the FDA-approved combination for endometrial cancer, pembrolizumab, and TKI lenvatinib, is being evaluated in a single-arm phase II trial and the primary endpoint analysis is estimated to be completed by July 2023 (NCT04865887, Table 2).
In contrast to the above mentioned combination strategies tested in the overall previously treated R/M cervical cancer population regardless of PD-L1 status, the anti-PD-1 sintilimab was tested in combination with the multikinase inhibitor anlotinib in a phase II trial, demonstrating its safety and efficacy as second-line or later therapy just for R/M CC patients expressing PD-L1 (Table 1). Interestingly, an exploratory analysis, evaluating other prognostic and predictive biomarkers beyond PD-L1, showed a significant correlation between altered PI3K/AKT signaling and KMT2D with the response, and a negative association of STK11 and/or JAK2 with PFS [55].
Novel Immunotherapeutic Strategies to Complement or Replace ICIsThe immuno-oncology is rapidly evolving, and a wide range of anticancer drugs with different mechanisms of action are under investigation beyond the immune checkpoint blockade and ADCs. Specifically, the current pipeline in the CC field mainly includes the investigation of adaptive cell therapy (ACT) and the development of cancer vaccines targeting HPV. Those new therapeutic approaches are designed to enhance the immune anticancer response, thus underscoring the urgent need of a deeper knowledge of the TME and its impact on therapeutic response.
Tumor-Infiltrating LymphocytesA novel immunotherapeutic approach that recently entered the clinic is the use of ACT. Three distinct ACT techniques were developed, with the common aim to stimulate the T cell response within the TME. Non-engineered tumor-infiltrating lymphocytes (TILs) were the first method studied. It consists of T cell extraction directly from the tumor site, ex vivo expansion, activation, and finally re-transfection in the patients [56]. LN-145 is a ready-to-use TILs therapy, which requires the previous administration of a non-myeloablative lymphocyte-depleting preparative regimen before the cell transfer, and the following infusion of interleukin-2 (IL-2). This autologous ACT approach showed promising results, both in the first line and in the subsequent settings (Fig. 1).
In the upfront setting, its efficacy was tested in combination with ICIs, showing striking results in terms of efficacy, and thus potentially representing the best-in-class immunotherapy-based combination strategy. LN-145 in addition to pembrolizumab demonstrated indeed a safety profile and antitumor activity with a reported ORR of 57% (95% CI, 28.9, 82.3) from the C-145–04/innovaTIL-04 trial, enrolling a cohort of chemo naïve CC patients (Table 3) [57].
LN-145 yielded further impressive results also as a single agent in the cohort of R/M CC patients who progressed on or after the upfront treatment. Preliminary results after a median of 3.5 months showed an ORR of 44%, with 11 out of the 12 responders still maintaining their responses at the time of the analysis (Table 1) [58].
Beyond the simple isolation of TILs from tumor samples, a technique to improve the specific recognition of T cells has further developed, through the genetic engineering of T cell receptor (TCR), which is highly specific for the recognition of MHC-restricted peptides [59]. This approach has been deeply studied in the HPV-associated CC subpopulation by several trials investigating the role of different MHC-restricted epitopes of E6/E7 oncoproteins. The first-in-human phase I/II study investigating the T cell therapy rescripted to an epitope of E6 did not show any tumor responses among the 6 patients enrolled in the trial [60]. Yet, a phase II trial generating T cells with HPV-oncoprotein reactivity showed an ORR of 28%, and, more interestingly, prolonged tumor responses were observed regardless of tumor histology (Table 1) [61]. A clinical trial with a higher avidity TCR, targeting the E7 oncoprotein is ongoing to further explore this approach (NCT02858310, Table 2).
Moving forward, the more recent TILs-based approach that entered the clinical setting was the chimeric antigen receptor (CAR) T cell therapy. In this case, T cells are engineered to recognize the tumor-cell surface antigens in an MHC-independent manner, thus overcoming one of the most important mechanisms of tumor immune escape, represented by the downregulation of MHC on cancer cell surfaces [59]. Clinical trials are now ongoing to investigate the applicability of this new treatment strategy even in the CC field, targeting different antigens, including CD22, GD2, PSMA, Muc1, or mesothelin (NCT04556669, NCT03356795, Table 2).
HPV-Related CC Population: Therapeutic Vaccines and the Transforming Growth Factor-Beta (tgf-β) Signaling PathwayOther therapeutic approaches were developed for the HPV-related subpopulation, targeting pathways and antigens used by HPV to evade immune surveillance and promote tumor growth. E6 and E7 are the two major oncoproteins mainly involved in driving the CC cells toward oncogenesis, by orchestrating all the hallmarks of cancers, including uncontrolled replication, tumor angiogenesis, invasion, and progression, through the unrestricted telomerase activity, along with the suppression of apoptosis [62]. Thus, therapeutic vaccines targeting E6/E7 oncogenes have represented an attractive tailored strategy for HPV-related cancers to enhance immune response driven by the concurrent blockade of the PD-1/PDL-1 axis. Several trials are currently investigating this combination strategy and preliminary safety and efficacy data were recently reported showing conflicting results. Positive results were observed in phase I/II trial investigating pembrolizumab in combination with GX-188E, a DNA vaccine encoding an E6/E7 fusion protein of HPV16-18 and linked with the Fms-like tyrosine kinase-3 ligand (FLT3L), with increasing antitumor response by stimulating the proliferation of hematopoietic progenitor cells. Significant activity was observed regardless of PD-L1 status, with observed ORR of 31.7% and 25% for the overall HPV16-18 population and the PD-L1-positive subgroup (Table 1) [63]. Accordingly, similar results were achieved in a heavily pretreated, HPV-16 positive, CC population with VB10.16, another therapeutic DNA vaccine encoding the E6/7 fusion protein of HPV16 and linked to the CCL3L1 chemokine via a dimerization module. In a pre-planned interim analysis of a phase II study evaluating the combination of atezolizumab and VB10.16 an overall ORR of 21% was observed, with encouraging clinical activity irrespective of PD-L1 status (ORR of 27% and 17% in the PD-L1-positive and negative population, respectively) [64]. In contrast, the DNA vaccine containing plasmids for E6 and E7 oncogenes for HPV-16/18 and interleukin-12 (IL-12) adjuvant, given in combination with durvalumab failed to demonstrate clinical activity. In the phase II trial evaluating this combination therapy in HVP16/18 related cancers, only one out of twelve patients enrolled in the CC cohort achieves a partial response, thus leading to the study discontinuation for futility. Notably, despite the low ORR, a clinically meaningful disease control rate was observed, and correlative studies are ongoing to further characterize the subgroup of CC patients with prolonged disease control without clinical responses (Table 1) [65]. Overall, DNA vaccines associated with ICIs were well tolerated, with a low incidence of grade ≥ 3 TRAEs (4% with GX-188E [63] and 23% with MEDI0457 [64]) and without any new treatment-emergent AEs compared to prior reports of these agents individually. AESI related to MEDI0457 were observed, including localized reaction and extremity pain at the injection site, none of these grade ≥ 3. The single-arm, phase II ongoing trial evaluating cemiplimab in combination with ISA101b is awaited to clarify the effectiveness of this combination approach (NCT04646005, Table 2). However, it must be pointed out that ISA101b is a structurally different vaccine because of its peptide-based nature. It is composed of long synthetic peptides from the E6/E7 HPV16 that are engineered to be delivered with adjuvant agents to stimulate the adaptive immune system, thus probably inducing a less potent immune response compared to therapeutic DNA vaccines.
Another attractive approach under evaluation in the HPV-selected CC population is the co-targeting of the PD-1/PD-L1 axis and the TGF-β pathway. The first-in-class bifunctional fusion protein Bintrafusp-alfa (M7824) is a new therapeutic drug consisting of two parts: the extracellular domain of TGF-β receptor II and an anti-PD-L1, linked by a flexible linker [66]. Data from phase 1 and phase 2 studies investigating its safety and efficacy in a pretreated, ICIs–naive, R/M CC population are encouraging, showing ORR of 28.2%, mDoR of 11.7 months and mOS of 13.4 months (95% CI, 5.5 to NR; Table 1). Also, toxicity was manageable, without any new safety signal different from previous reports for anti-PDL1 agents and TRAEs known to be related to TGF-β inhibitors (Grade ≥ 3 TRAEs observed: skin lesions, colitis, asymptomatic lipase increase, and gastroparesis with hypokalemia)[67].
Comments (0)