
Remember me






A 53-year-old man, 168 cm tall, weighing 60.4 kg (body mass index 21.4 kg/m2), and suffering from difficulty in swallowing since his mid-teens, presented for treatment of the dysphagia. His symptoms worsened in winter and had progressively worsened over time. His medical history included autoimmune hepatitis, and he had no family history of gastrointestinal tract diseases. Chest X-ray showed mediastinal enlargement and presence of air-fluid levels in the thoracic esophagus (Fig. 1). He underwent upper gastrointestinal endoscopy along with biopsy, which showed a dilated esophagus with food residue and constriction of the esophagogastric junction. He was diagnosed with achalasia type 2 according to the Chicago classification, indicating that his esophagus did not have effective movement [6]. He was scheduled for endoscopic myotomy of the esophagus under general anesthesia. Preoperative computed tomography imaging revealed the shape of the esophagus, with an enlarged upper part and narrowed lower part containing much residue (Fig. 2A). Additionally, he was found to have a left renal tumor and was scheduled for renal cancer surgery before esophageal myotomy (Fig. 2B).
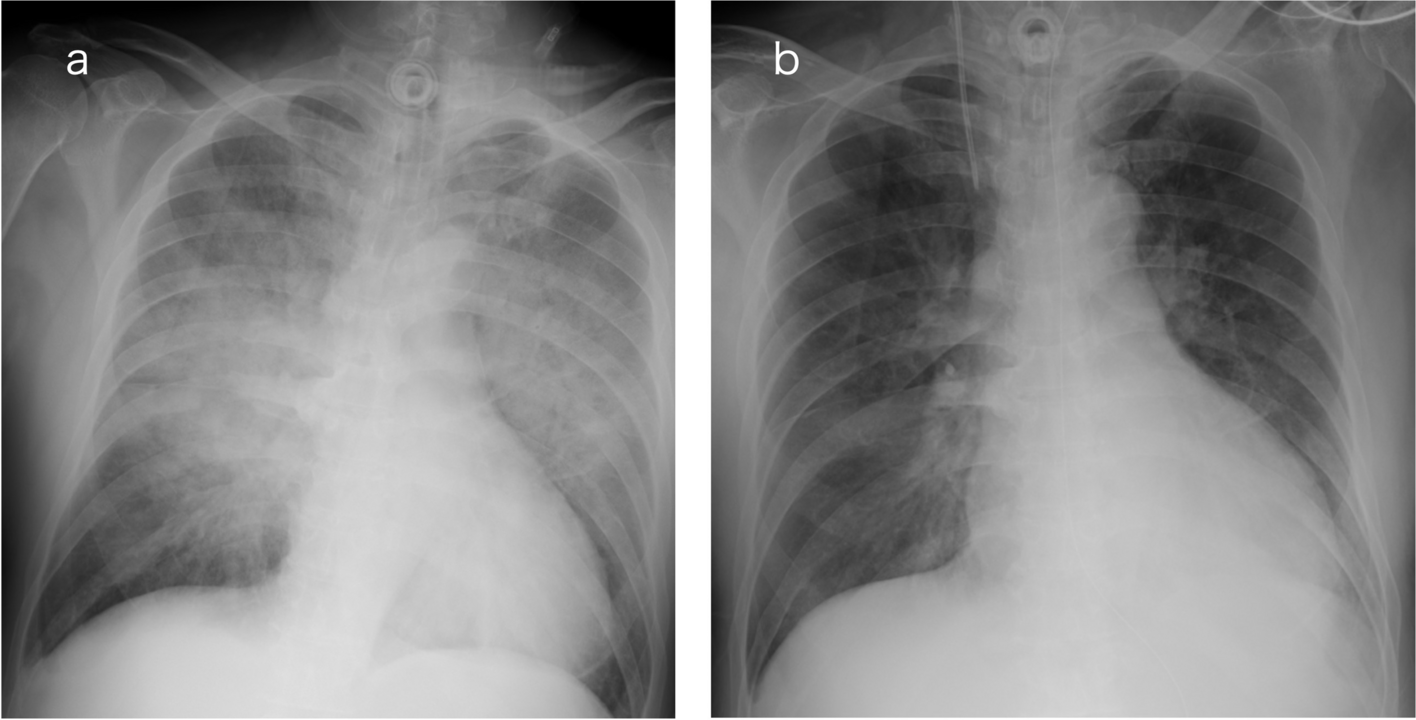
Fig. 1
Chest X-ray demonstrated enlargement of the mediastinum (white arrows) and presence of air-fluid levels in the thoracic esophagus (yellow arrowhead)
Fig. 2
A Axial computed tomography (CT) image showing the enlarged esophagus filled with residue (arrow). B Coronal CT image showing dilation of the upper part and narrowing of the lower part of the esophagus, presenting a bird beak shape (white arrow). The left renal tumor is also seen (yellow arrowhead)
When he entered the operation room for the renal surgery, his vital signs were a heart rate of 74 beats/min, blood pressure of 132/92 mmHg, and SpO2 of 98%. Before induction of anesthesia, a 14-Fr stomach tube was inserted to a depth of 55 cm from his left nostril. Even though he had been fasting for 15 h, approximately 300 ml of residue was aspirated via the tube. Subsequently, after preoxygenation with 100% oxygen for 5 min, rapid sequence induction (RSI) was performed in the supine position with 110 mg of propofol, 60 mg of rocuronium bromide, 0.2 μg/kg/min of remifentanil, and 0.1 mg of fentanyl, using video laryngoscopy. Although the cricoid pressure (CP) maneuver was not applied along with RSI, intubation was successfully performed without regurgitation. Laparoscopic nephrectomy was performed in the right lateral recumbent position. Anesthesia was maintained with air, oxygen, desflurane, and remifentanil. To prevent regurgitation in case of bucking and elevated esophageal pressure due to pneumoperitoneum and the intraoperative position, rocuronium bromide was intermittently administered under neuromuscular monitoring using acceleromyography. The train of four (TOF) count was used to monitor the state of muscle relaxation. The total blood loss and urinary volume were 2 ml and 250 ml, respectively. The volume of infusion was 2298 ml during anesthesia. At the end of the operation, chest X-ray showed that the stomach tube had formed a loop in the dilated esophagus and did not reach the stomach (Fig. 3). After turning the patient over to the supine position and before extubation, the contents of the esophagus were again aspirated via the tube, although only minimal residue was obtained. The 5-HT3 receptor antagonist, ondansetron, was administered to prevent postoperative nausea and vomiting (PONV). Since the TOF count was 1 at the end of the surgery, 200 mg (3.3 mg/kg) of sugammadex was administered, resulting in recovery of the TOF count to 4. Finally, his trachea was extubated after recovery of spontaneous respiration without regurgitation at the supine position. The operation time was 4 h 33 min, and anesthesia time was 5 h 36 min.
Fig. 3
Chest X-ray image demonstrating enlargement of the mediastinum (white arrows). The stomach tube had formed a loop in the dilated esophagus (yellow arrowheads)
At his exit from the operation room, the patient’s vital signs indicated a heart rate of 63 beats/min, blood pressure of 83/50 mmHg, and SpO2 of 99%. He was postoperatively observed in the intensive care unit (ICU). His postoperative pain was well controlled with 1 ml/h of patient-controlled analgesia consisting of 25 μg/ml fentanyl and 125 μg/ml droperidol, without PONV. He was discharged from the ICU on postoperative day 1, and his subsequent postoperative course was uneventful.
Comments (0)