We encountered two cases of NPPE after tracheostomy. Because NPPE usually develops with upper airway obstruction, it rarely develops in a secured airway such as that after a tracheostomy. NPPE develops when the increased inspiratory effort associated with upper airway obstruction decreases the intrathoracic pressure. A sudden drop in intrathoracic pressure creates a pressure differential within the blood vessels and alveoli, where the fluid moves from the pulmonary veins to the pulmonary interstitium, suggesting that NPPE is caused by hydrostatic pressure differences between pulmonary capillaries and interstitium rather than increased permeability of the pulmonary capillaries [1]. Lower edema fluid/plasma protein ratio reported in patients with NPPE than those with high-permeability edema also supports this hypothesis [3,4,5].
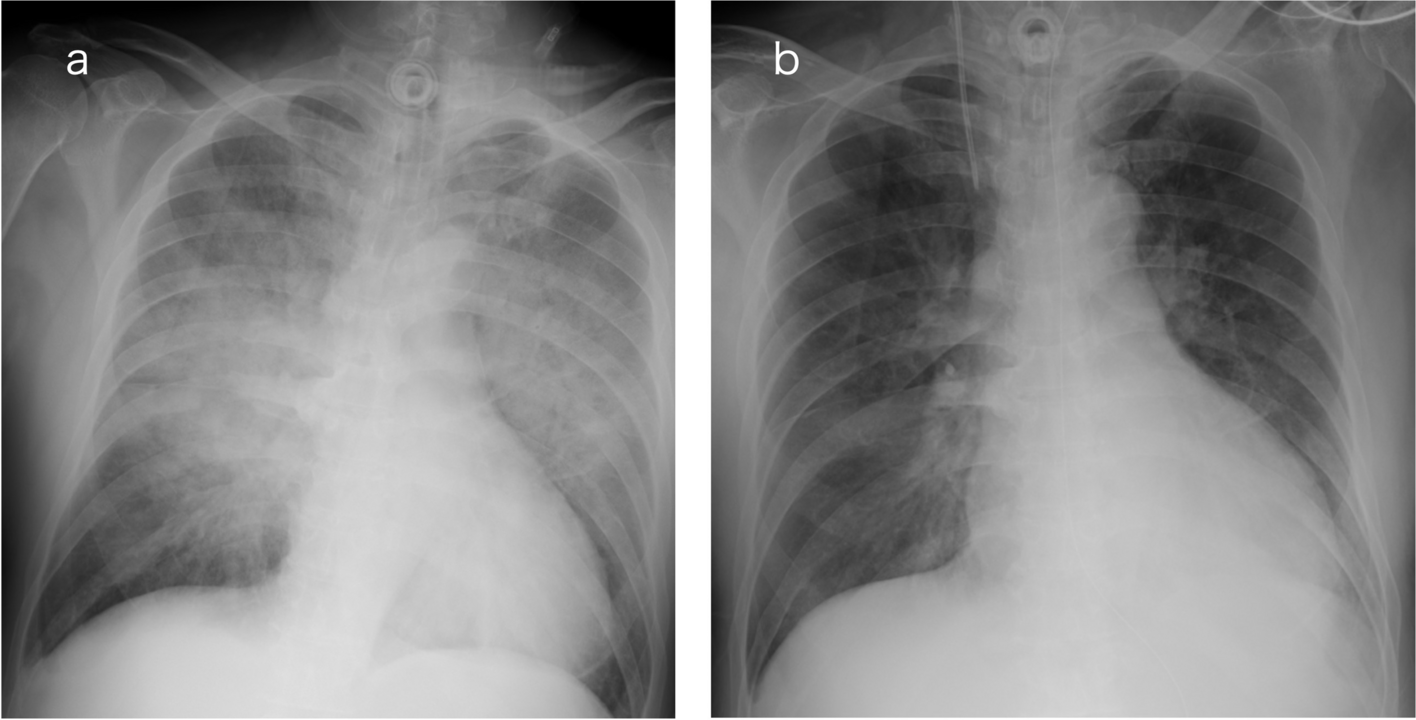
The diagnostic criteria for NPPE include (1) upper airway obstruction; (2) sudden onset of respiratory difficulty, hypoxia, and hypercapnia; (3) presence of frothy sputum; and (4) chest radiographic findings showing diffusely increased density, widened vascular shadows, and bilateral, central alveolar, and interstitial infiltrates [6]. Although our cases lack mechanical upper airway obstruction as commonly observed after extubation, they suggest that similar conditions can occur both mechanically and functionally, even in patients with secured airways.
In Case 1, sputum caused mechanical airway obstruction of the tracheostomy tube. On the other hand, Case 2 had difficulty breathing and developed tachypnea due to withdrawal syndrome, although secretions in the trachea unlikely caused airway obstruction. Ineffective ventilator triggering occurs when the next inspiratory effort begins before the expiratory outflow is completed under positive-pressure ventilation [7]. In this case, the high PSV pressure setting caused hyperinflation, which, combined with high airway resistance (due to tracheostomy airway), resulted in a prolonged expiratory time. As a result, the next inspiratory effort was initiated before the expiration was completed. Still, it did not reach the flow trigger sensitivity, leading to an ineffective triggering, which caused the negative intrathoracic pressure. Tachypnea and high PSV pressure may have caused ineffective triggering, resulting in intense negative endotracheal pressure. With residual expiratory flow, strong inspiratory effort is required to meet the ventilator flow-triggered air delivery criteria. NPPE can occur due to functional airway obstruction, even without mechanical occlusion. Although rare, a similar case of NPPE after tracheostomy has been reported [8]. They noted that acute or chronic obstruction resolves after tracheotomy can lead to severe dyspnea with NPPE, as seen in Case 2. Furthermore, a pediatric study reported that children have higher thoracic compliance, which allows decreased airway pressure to greatly affect intrathoracic pressure [9]. They observed that NPPE developed in 7% of children with upper airway obstruction. This is higher than the recently reported 3% incidence of NPPE in adults with upper airway obstruction [10].
The most crucial treatments for NPPE include relieving the upper airway obstruction and administering positive-pressure ventilation [2]. Several studies have reported that NPPE resolves within 24–48 h in most cases [1, 2, 11]. Because NPPE results from hydrostatic rather than increased permeability edema, it responds well to positive-pressure ventilation and improves rapidly. The two cases we encountered illustrated this point. If pulmonary edema does not improve with these treatments, the differential diagnoses should include acute heart failure, acute respiratory distress syndrome, aspiration pneumonia, or pulmonary thromboembolism [12].
In conclusion, we encountered two cases of NPPE after tracheostomy due to mechanical and functional airway obstruction. These cases demonstrate that NPPE should be considered even in patients with an airway secured with a tracheostomy.







Comments (0)