The female urethra is short, approximately 3.5 to 5 cm [1, 2], and insertion of a urethral catheter is generally easier in women than in men when the urethral meatus can be visualized [2]. However, the meatus is often difficult to visualize, which can lead to catheter misplacement in the vagina [1,2,3]. The absence of urinary outflow is an indication that a catheter may be in the vagina [2, 3]. However, in the present patient, catheter misplacement was not detected in a timely manner because of the assumption that had the catheter been misplaced in the vagina, no urinary outflow would have occurred. Had the problem not been discovered in our patient, unnecessary laboratory tests and treatments would have been conducted to address the subsequent lack of urinary output. Therefore, this patient represents a didactic case illustrating that even if urinary outflow is observed during female urethral catheterization, catheter misplacement in the vagina cannot be ruled out. This potential issue cannot be ignored by anesthesiologists who use urinary output for perioperative management. Even if urinary outflow is observed during female urethral catheterization, if the urethral meatus cannot be identified upon catheter insertion, or if drainage stops, catheter misplacement in the vagina must be ruled out or verified by pelvic examination or bladder ultrasound.
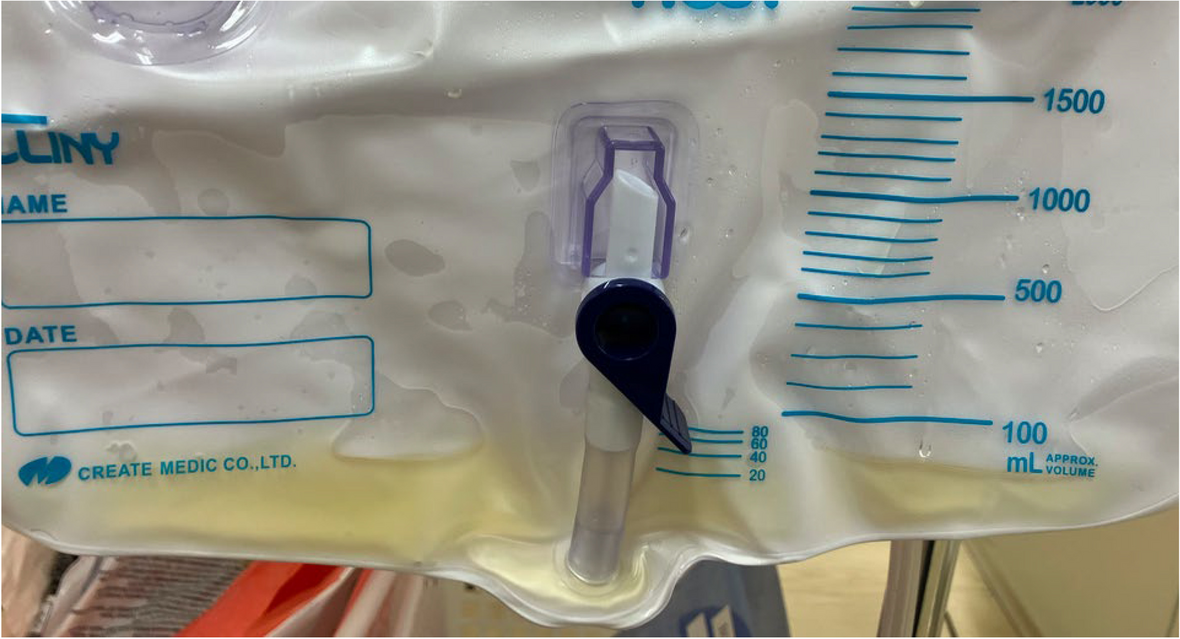
After discovering that the urethral catheter has been placed in the vagina in the patient, we considered the possibility that vaginal discharge which was characteristic of urine had drained. However, vaginal discharge in older adults is normally minimal unless vaginitis is present, which causes increased purulent vaginal discharge [6]. After consulting an obstetric gynecologist, we confirmed the drainage fluid to be urine and not vaginal discharge based on the large volume and pale-yellow appearance.
This led us to ask the following question. Why was urine retained in the vagina at the time of urethral catheterization? Reportedly, a urogenital fistula (UGF) [7, 8] and vesicovaginal reflux (VVR) [9,10,11] can cause urine to enter the vagina. Our patient had no history of urinary incontinence suspected to be congenital UGF and no history of pelvic surgery, malignancy, or radiotherapy that could have caused acquired UGF [7, 8]. In addition, the absence of persistent urinary outflow during the initial urethral catheterization essentially ruled out UGF. In contrast, VVR is defined as the reflux of urine into the vaginal vault during voiding [9] and has been reported as an underestimated cause of urinary incontinence in adult females [10]. Labial adhesions or tightly opposed labia majora may cause backflow into the vagina by preventing the passage of urine [11]. In the present case, upon removal of the second urethral catheter, the tightly opposed labia majora prevented complete voiding in the supine position in which the legs were in a neutral position (not abducted), and the urine flowed down the perineal and buttock skin. In addition, the patient experienced functional urinary incontinence daily and remained in the supine position with the legs in neutral after the fracture. Therefore, VVR likely occurred during voiding while the patient was in this position, and urine remained in the vagina because the patient remained in the position until surgery.
Moreover, we recognize human error in that the urethral catheter was misplaced in the vagina because of catheter insertion under conditions in which visualizing the urethral meatus was difficult. This difficulty may have been precipitated by the anatomical shift of the meatus to the vicinity of the vaginal opening because of postmenopausal vaginal atrophy [5] and inadequate positioning during catheter insertion. The patient was under general anesthesia; therefore, an adequate supine frog-legged or lithotomy position might have been a better choice for visualization of the meatus. In cases where the meatus is difficult to visualize despite efforts to adjust positioning and lighting, proper catheter insertion can be managed by the clinician inserting a finger into the vagina as a guide [1, 2, 4, 5]. In addition, bladder ultrasound is easy to perform in the operating room and useful for confirming the correct position of the urethral catheter in the bladder [12]. These measures would help prevent catheter misplacement and ensure correct catheter placement. If multiple catheter insertion attempts fail, a urologist or gynecologist should be consulted.
In summary, we encountered an older adult patient in whom the urethral catheter was misplaced in the vagina. Detection was delayed because urinary outflow had been observed during the catheterization. Even if urinary outflow is observed during female urethral catheterization, catheter misplacement in the vagina cannot be ruled out. Therefore, catheter misplacement in the vagina must be ruled out in cases in which the urethral meatus cannot be identified upon insertion of the catheter or drainage stops.







Comments (0)