
Remember me






We were planning to compare the use and non-use of a stylet and compare four differently shaped stylets in the ease of tracheal intubation in neonates, but we felt that it would be more ethical to carry out first, a preliminary study in a manikin of a neonate, because the efficiency of some shapes of stylets were predicted to be less effective. The study protocol was submitted to the research ethics committee which informed us that the study did not require a formal review, because this study was not a study on human subjects. Written informed consent was obtained from all the participants.
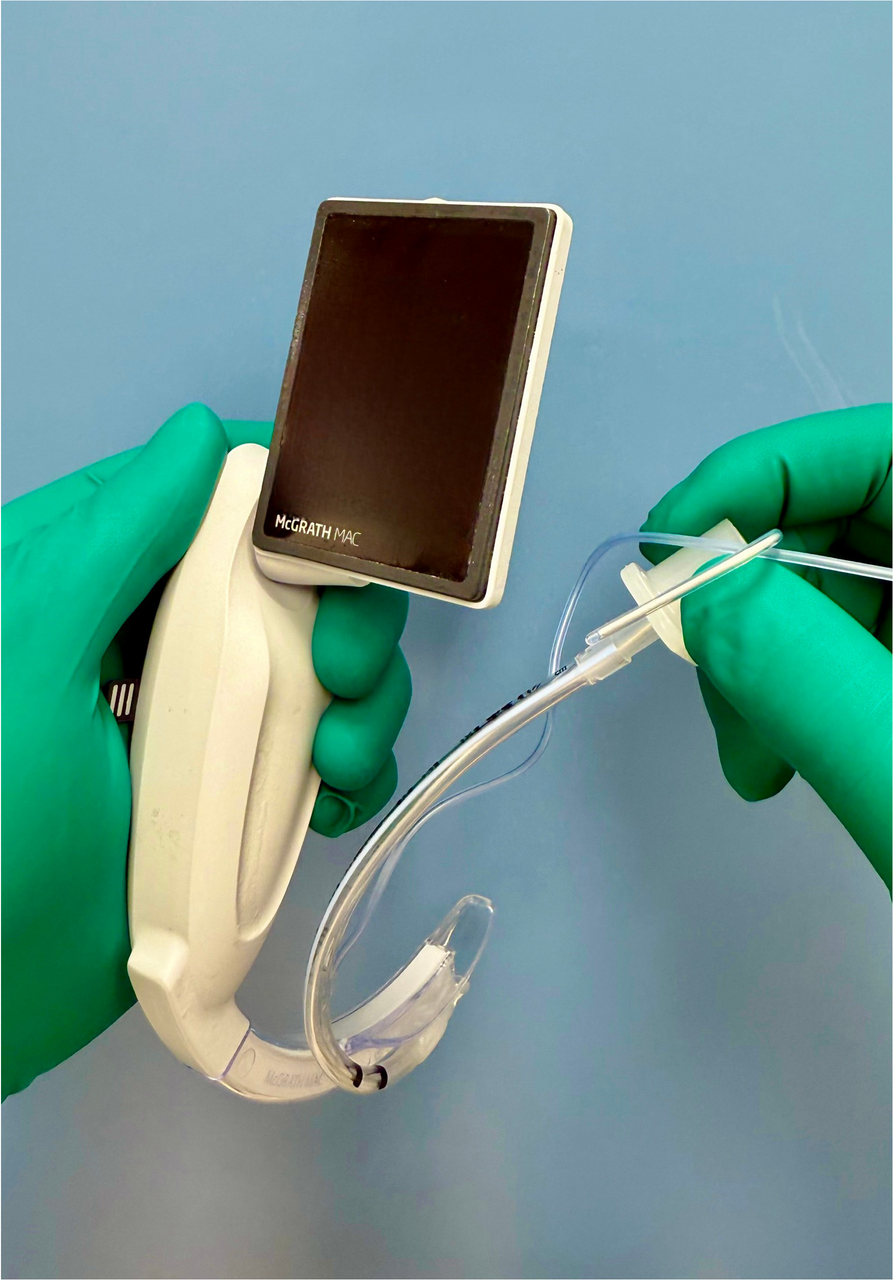
As a randomized controlled cross-over design, the use of four differently shaped stylets were compared with no stylet in the ease of tracheal intubation in a manikin of a neonate (Laerdal® Medical, Stavanger, Norway). Twenty-five anesthesiologists (3 specialists, 11 senior residents, and 11 junior residents) with at least 1 year of experience in pediatric anesthesia used a McGrath® MAC videolaryngoscope (Covidien, Medtronic, Tokyo, Japan) blade 1 for tracheal intubation, with one of four differently shaped stylets (C-shaped, J-shaped, hockey stick-shaped, and double C-shaped) or without a stylet. The shape of stylet (tracheal intubation stylet (2.0-mm OD, 255 mm), Smith Medical, Minneapolis, USA) is defined as follows: the C-shaped stylet follows the curve of the laryngoscope blade so that the curve looked like the letter C, the J-shaped stylet has its tip formed into the letter J, the hockey stick-shaped stylet has the tip bent at a 90-degree angle, and the double C-shaped stylet (Fig. 1) has the distal part of the tracheal tube bent along the shape of the blade, with a 45-degree bend at the connection between the blade and handle of the McGrath® MAC [12]. A 3.5-mm ID tracheal tube with a cuff (Shiley™ oral/nasal endotracheal tube with intermediate cuff, Covidien, Mansfield, USA) was used for all the intubation attempts, and a water-soluble lubricant was applied to its cuff before each use. The order of intubation methods was randomized.
Fig. 1
Double C-shaped stylet. The stylet has the distal part of the tracheal tube bent along the shape of the blade, with a 45-degree bend at the connection between the blade and handle of the McGrath® MAC videolaryngoscope
The primary outcome measure was time to tracheal intubation on the first attempt, and the secondary outcome measure was the success rate of tracheal intubation at the first attempt. The time to tracheal intubation was defined as the time from when the tip of the blade entered the oral cavity until the anesthesiologist declared that the tube was inserted to the trachea. One of the investigators (KM) assessed the position of the tracheal tube, and if the tube was not inserted in the trachea, it was judged failure. We also judged that tracheal intubation failed, if it took more than 45 s [13]. This cut-off valve was based on our previous study of children under 2 years age, in which the median time to tracheal intubation using a McGrath blade 1 and a C-shaped stylet was 45 s. If tracheal intubation failed at the first attempt, another attempt was allowed.
Friedman’s two-way analysis of variance was used to compare the time to intubation between five different methods, and if this indicated a significant difference, Wilcoxon rank sum test was used to compare the intubation time between no use of a stylet and each of differently shaped stylet. P < 0.05 was considered as significant. 95% confidence intervals for median difference, with and without the use of a differently shaped stylet, were also calculated.
Power analysis was carried out for the primary outcome measure (time to tracheal intubation on the first attempt). In our previous studies of children in whom the McGrath® MAC blade 1 and a C-shaped stylet was used, the mean time (and the standard deviation) was 38 (7.4) s [13] and 40 (12.9) s [14]. From these studies, we estimated the mean time with a C-shaped stylet would be 40 s, with the standard deviation of 12 s. We considered that the difference of 20% (that is 8 s) in intubation time would be minimally clinically meaningful. To detect this difference, with a power of 0.8, and P = 0.05, the minimum of 21 participants would be required. To obtain a reasonably accurate estimation of the difference between groups, we decided to study 25 participants.
Comments (0)