
Remember me






Low circulating blood volume decreases venous pressure [3], and the use of a large bore needle may pose a risk to posterior vein wall penetration [4]. Blaivas et al. reported that the cause of mechanical complication during US-IJV may be related to double-wall penetration [5]. The needle advanced behind this anatomic structure may damage the artery and/or lung. Some guidelines recommend checking the guidewire position before inserting a dilator to prevent subsequent lethal complications [3, 6, 7]. The guidewire position should be confirmed in both the short- and long-axis views [7, 8]. However, in the present case, the guidewire position was confirmed only in the short-axis view. Therefore, the guidewire penetrating the internal jugular vein could not be confirmed. Wakabayashi et al. reported that in an US-IJV, the starting sticking point should be at least 5-cm cephalad from the clavicle to confirm guidewire position in the long-axis ultrasound view [8]. In adult men, the apex of Sedillot’s triangle lies approximately 5-cm cephalad from the clavicle. Therefore, if puncture is started at the apex of Sedillot’s triangle, the guidewire position can be confirmed in the ultrasound long-axis view. However, in the present case, the starting needle-sticking site was at the midpoint of the Sedillot’s triangle, which was insufficient to confirm the guidewire position in the long-axis view. Starting the puncture from the apex of Sedillot’s triangle is called the “high approach,” whereas puncturing from caudal to the midpoint of Sedillot’s triangle is called the “low approach” [9] (Fig. 3). The present case suggests that the high approach is more advantageous than the low approach in that the guidewire position can be reliably confirmed. In the case of a patient with short neck, the use of short-length needle (32–38 mm) for internal jugular venous catheterization is recommended. This needle length is sufficient to puncture the internal jugular vein, and the needle may not reach the blind zone behind the clavicle by using the high approach.
The selection of the optimal needle-sticking site for the anatomic landmark technique has been discussed along with its success rate. It has been shown that US-IJV can be performed in any neck site if the internal jugular vein can be identified. Troianos et al. recommended that the internal jugular venous puncture should be performed in a direction that does not overlap with the common carotid artery to avoid accidental arterial injury [10]. However, arterial injury during US-IJV occurs in the common carotid and subclavian arteries [3, 11]. Therefore, selecting techniques that do not cause double-wall penetration is more important than selecting the optimal needle-sticking site for US-IJV. The authors focused on the sternocleidomastoid muscle, which was used as an anatomic landmark for traditional landmark technique. However, for performing US-IJV, the sternocleidomastoid muscle is not a landmark but an obstacle. This can be attributed to the fact that the thick muscle belly of the sternocleidomastoid muscle is considered a risky needle-sticking site that can interfere with puncture and dilator insertion, which may cause kinking of the guidewire. The high approach recommended in anatomic landmark technique may also be one of the best needle-sticking sites for US-IJV, as it confirms the guidewire position using long-axis ultrasound view and allows easy handling of the needle and smooth insertion of the dilator in Sedillot’s triangle.
The methods used to detect occasional arterial puncture include pressure measurement of the catheter and blood gas analysis [3, 6]. In the present case, the anesthesiologist observed saline dripping through the catheter to confirm the catheter tip location. However, in patients with shock, hypotension, or in whom the cannula tip is in contact with the vein wall, the arterial pressure should be low enough to allow easy spontaneous dripping. Pressure monitoring may also be less reliable in patients with low blood pressure.
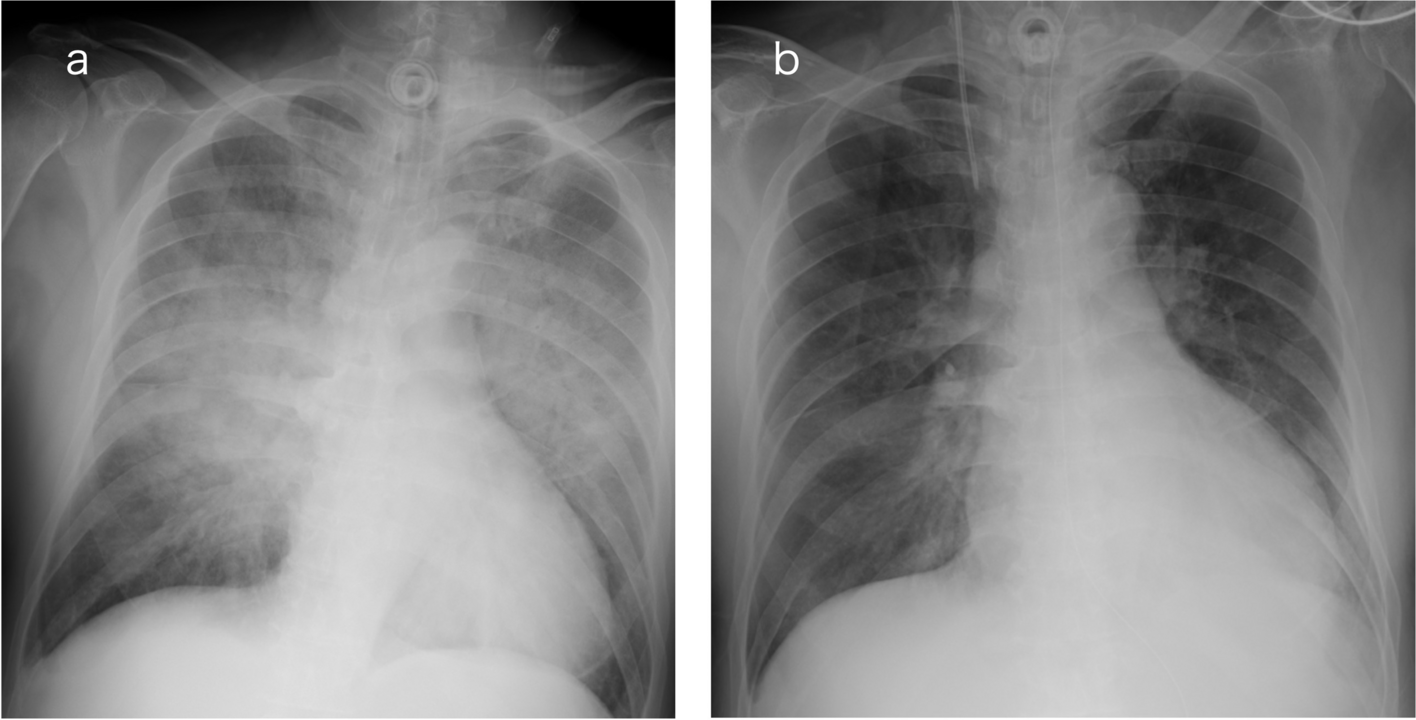
After central venous catheter placement, the location of the catheter is usually confirmed by chest radiography. The inappropriate catheter placements include misplacement into a small vein and extra-venous misplacement. Essentially, the radiographic film should be read on vascular anatomy. Figure 4 shows the small veins tending catheter misplacement. When reading chest radiographs, it is crucial to consider these locations to determine if the catheter was simply misplaced in a small vein or outside a vein. Once it is determined that the catheter is placed at an inappropriate location, an immediate CT or MRI is recommended to determine its exact location and select the befitting treatment for misplacement of a central venous catheter [12].
Fig. 4
Schematic representation of cervical and thoracic veins for possible misplacement of central venous catheters. a Frontal view. b Lateral view showing ① right internal thoracic vein, ② left internal thoracic vein, ③ pericardiophrenic vein, ④ azygos vein, ⑤ right inferior thyroid vein
We experienced a case of central venous catheter misplacement into the right subclavian artery during ultrasound-guided right internal jugular venous catheterization. We recommend the use of the high approach for internal jugular venous catheterization, which allows confirmation of the guidewire position.
Comments (0)