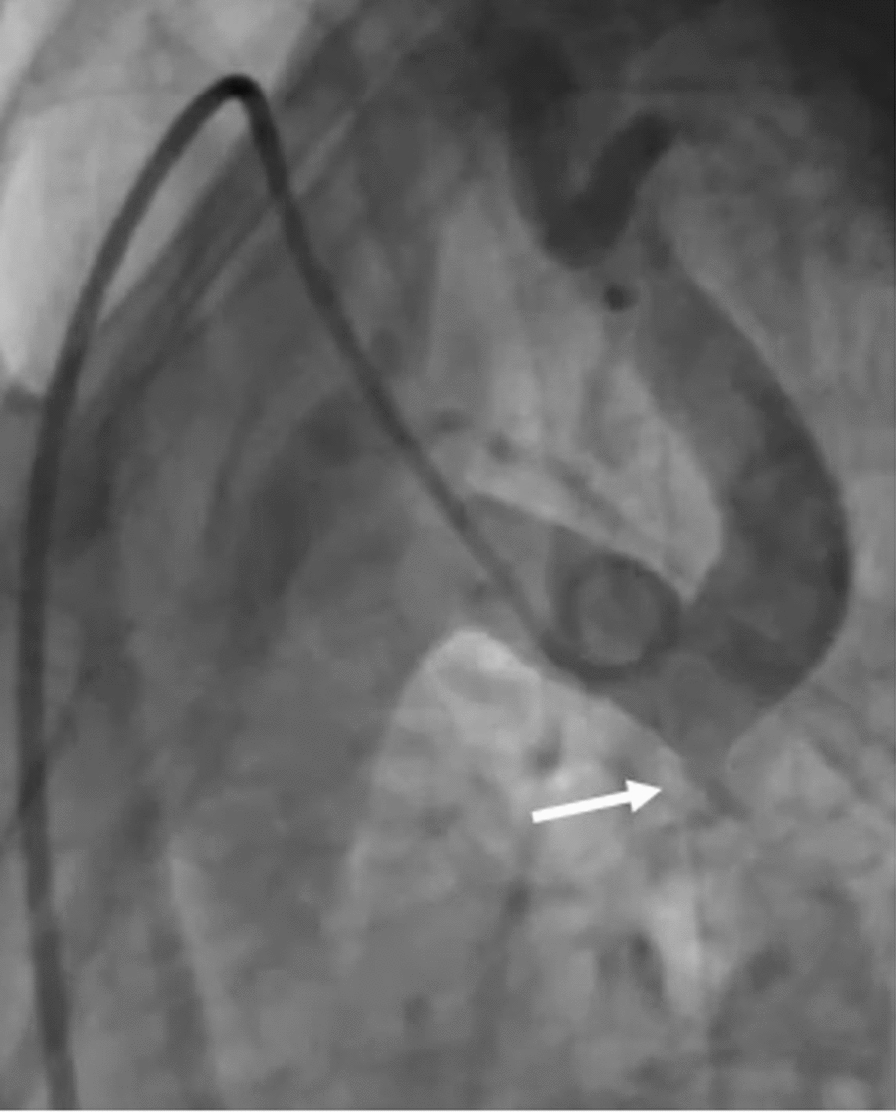
There are no specific early signs in PH. The most common symptom is dyspnea especially on exertion; however, it is usually neglected till progression of disease happens with more symptoms developed like chest pain or syncope. As a result of that, PH symptoms deteriorate till diagnosis with delay over 2.8 years [16]. After diagnosis of PH, more than 75% of PH patients have advanced symptoms with complications like pulmonary vascular remodeling and right ventricular failure. Till now, the best available tool in diagnosis of PH is right heart catheterization “RHC.” But because it is an invasive tool so developing new non-invasive diagnostic tools like biomarkers might be important to avoid complications and the high cost of RHC [17].
Unfortunately, the available biomarkers used nowadays for diagnosis of PH are not specific and can be of diagnostic value in late stages of the disease, and they might be also affected by other metabolic functions. However, various biomarkers especially miRNAs are now developed and emerged as a good biomarkers in PH [18].
Our study found that miR-21 was significantly upregulated in patients with group 1 PH and when we compared miR-21 in group 1 PH with group 2, 3 PH and control, we found that there is a highly significant difference between group 1 and group 2 (P = 0.005) and between group 1 and control (P = 0.004) and a significant difference between group 1 and group 3 (P = 0.043). Also, we found that the cut off predictive value of miRNA 21 (≥ 1.55 µM ) has sensitivity (60%), specificity (95%), positive predictive value (94.7%) and negative predictive value (61.3%) with AUC (0.742). So, miR-21 might be used as a good biomarker to differentiate group 1 PH from group 2 and 3 PH.
Upregulation of miR-21 in patients with PAH is affected by hypoxia where HPASMCs had a 3-fold rise in miR-21 level. Bone morphogenic protein 2 “BMPR2” signaling leads to upregulation of miR-21. RhoB is targeted directly by miR-21, and this leads to suppression of its expression and activation of kinase which leads to endothelial dysfunction, inflammation and development of PH [19].
Also, Victoria et al. found that miR-21 integrates multiple pathogenic signals to regulate PH. Hypoxia, inflammation and BMPR2-dependent signaling upregulate miR-21 in the pulmonary vasculature, and this leads to Rho-kinase activation which modulates the development of PH in vivo [20].
Regarding miRNA-124, our study found that miR-124 was down-regulated in patients with group 1 PH and when comparing miR-124 level in group 1 PH with group 2, 3 PH and control, we found that there was highly significant difference between group 1 as compared to group 2 and control (P < 0.001) but no significant difference between group 1 and 3 group. The cutoff predictive value of miRNA 124 (≤ 1.58 µM) has sensitivity (86.7%), specificity (75%), positive predictive value (83.9%) and negative predictive value (78.9%) with AUC (0.789).
Decreased expression of miR-124 modulates fibroblasts phenotype of pulmonary artery, smooth muscle cells “SMCs” and endothelial cells outgrowth from pulmonary hypertensive patients and also miR-124 add-back reversed of these cell's phenotype [21].
Cell proliferation and PH were affected by different factors as the nuclear factor of activated T cells “NFAT” signaling pathway. NFAT activity is inhibited by miR-124 and leads to affection of dephosphorylation, nuclear translocation and NFAT-dependent transcription of IL-2 which shows the beneficial value of miR-124 in preventing PH. Also NFAT pathway was modulated by miR-124 through targeting nuclear factor of activated T cell cytoplasmic 1 “NFATc1,” calmodulin-binding transcription activator 1 “CAMTA1” and polypyrimidine tract-binding protein 1 “PTBP1.” Also, down-regulation of miR-124 in PASMCs and mice lungs was induced by hypoxia so PASMCs proliferation was inhibited by over expression of miR-124 [22].
Transcriptional products from miR-124 genes were examined by Hui Zhang et al., and he reported that PH patients have reduction in the transcription activity of miR-124 gene and that there is epigenetic changes happened due decreased miR-124 expression with the development of PH [23].
Zhang et al. found that miR-124 in patients with PAH was significantly down-regulated with down expression in PASMCs. Also, reduced miR-124 levels in patients with PAH and experimental PH models led to upregulation of polypyrimidine tract–binding protein 1 “PTBP1” by a high proliferative and migratory phenotype. [24].
One of the molecules of the family of transforming growth factor “TGF-β” is endoglin which is a membrane co-receptor. It is involved in vascular development, homeostasis, repair and disease and predominantly expressed by endothelial cells [25].
In our study, we found that expression of endoglin was increased in patients with group 1 PH with a highly significant difference between group 1 PH as compared to group 2 PH and control (P < 0.001) and a significant difference between group and group 3 PH (P = 0.011). Also, we found that a cutoff predictive value endoglin (≥ 1.5 ng/ml) has 93.3% sensitivity, 95% specificity, 96.6% positive predictive value and 90.5% negative predictive value with AUC (0.94), so endoglin might be used as a good biomarker for early diagnosis of group 1 PH and also to differentiate group 1 PH from group 2 and 3 PH.
There is high expression of endoglin in PAH lungs especially in the microvascular endothelial as compared to the lungs of control, and the intensity of expression was more in the sites of dysregulated angiogenesis called plexiform lesion in PAH. The increased concentration of endoglin in blood leads to endothelial dysfunction and proliferation. Endoglin is released from the sites of active remodeling by activation of activation of matrix metalloproteinase-14 “MMP-14” [13]. Expression of endoglin on vesicular endothelial cells is considered as an ancillary receptors for many super family ligand TGF as BMPR2 and serve as to modulate both BMPR2 and TGF-lysical association with activin like kinase receptor 1 “ACTLR-1” gene product [26]. Increased level of endoglin and the occurrence of PAH were due to highly oxidative stress in hereditary hemorrhagic telangiectasia [27]. Endoglin regulates activation and vasomotor tone of endothelial nitric oxide synthase “NOS” through binding with it [28].
In a study performed by Mohammed Noori Al-Dujaili et al., he reported that when comparing PAH patients with healthy subjects regarding endoglin levels, there was a significant difference between the 2 groups [29].
Also, the clinical study of Coral et al. found that the endothelial cells enriched high affinity TGF- receptor with upregulation of endoglin which led to vasculopathy in PAH [30].
In our study we found that levels of ADMA were elevated in group 1 PH with a highly significant difference (P < 0.001) between it and control however there was no significant difference between group 1 PH as compared to group 2 and 3 PH so it failed to differentiate between group 1, 2 and 3 PH.
One of the most important endothelium-derived vasoactive substances is NO which has a vital role in regulating vascular homeostasis and local vasomotor tone. Endothelial dysfunction occurred due to deceased levels of NO. NO is synthesized from L-arginine through the action of NOS. ADMA is an endogenous competitive inhibitor of NOS which blocks the action of NOS and considered a novel biomarker in various diseases such as hypercholesterolemia, coronary artery disease [31], peripheral arterial disease [32], chronic heart failure [33] and PH [34].
Inflammation, collagen deposition, oxidative stress and altered lung function were associated with increasing levels of ADMA. Also, there is a direct association between ADMA levels and obstructive lung diseases [35, 36].
In a study done by Juan Liu et al., he reported that elevated ADMA levels are associated with the presence and severity of PAH in connective tissue disease “CTD” patients, and levels of ADMA in the serum might be used as a valuable biomarker for early diagnosis of CTD-PAH patients [37].

Comments (0)