
Remember me
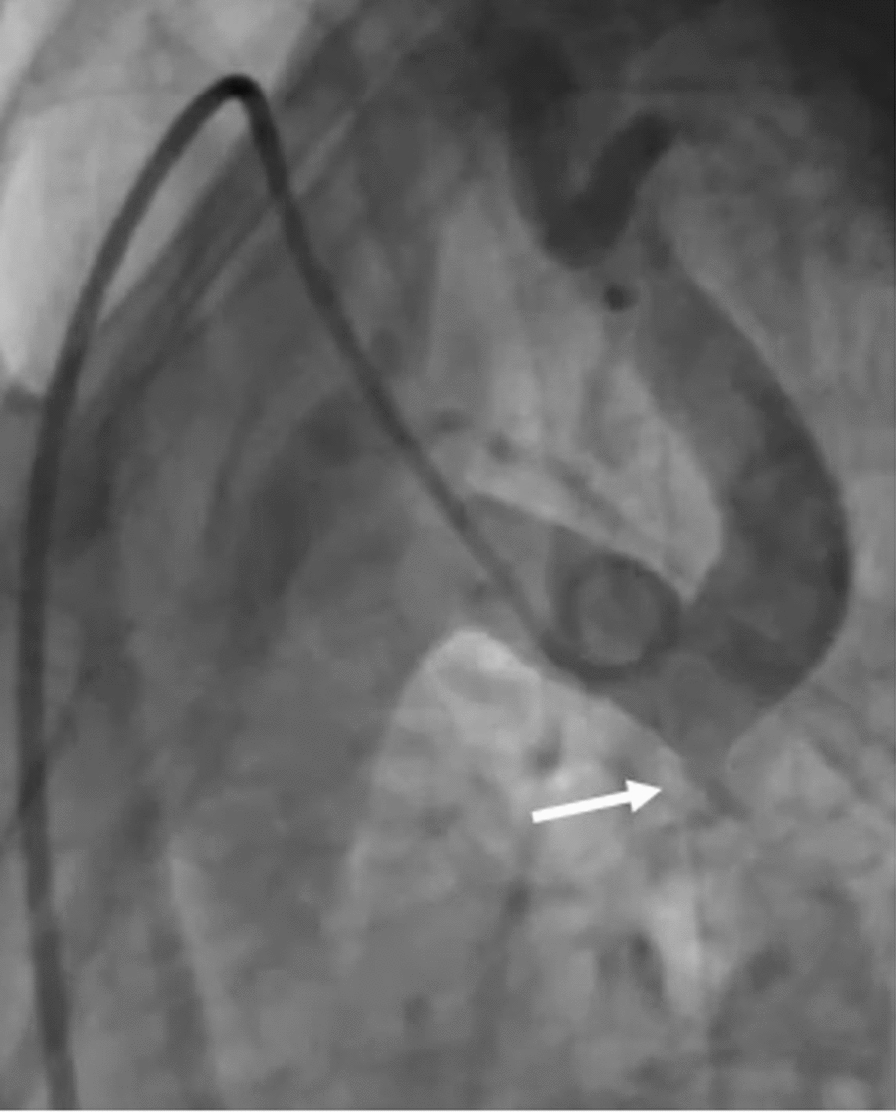
A 22-year-old lady was admitted to our cardiology unit with a diagnosis of Severe native CoA for percutaneous stenting. The patient was diagnosed with Turner’s Syndrome with Chronic Idiopathic thrombocytopenia purpura (ITP). She had refractory hypertension despite multiple antihypertensives. Echocardiography showed severe concentric left ventricular hypertrophy with bicuspid aortic valve with mild aortic stenosis. The gradient across the CoA segment was 90 mmg with diastolic tailing. We obtained right femoral artery access using a 5-French micropuncture set under ultrasound guidance. Additionally, we secured 6-French left femoral vein access for placing a temporary pacing lead. A 6-French right radial access was obtained to position a pigtail catheter in the aortic arch for angiographic guidance during stent placement. The initial femoral arterial pressure before the intervention was 80/60 mmHg, while the ascending aortic pressure was 170/70 mmHg, resulting in a gradient of 90 mmHg. The aortic arch angiogram from the right radial approach revealed severe post-subclavian CoA (Fig. 1). The pre-CoA segment measured 18 mm, while the post-CoA dilated segment measured 22 mm. We selected a stent diameter of 16 mm, approximately 80–90% of the pre-CoA segment diameter. A stent length of 40 mm was chosen to adequately cover the CoA segment while minimizing excessive protrusion into adjacent structures.
Fig. 1
Aortic arch angiogram from right radial route showed tight post-subclavian CoA
The CoA site was crossed from the femoral route with 0.35 Terumo wire with the Judkin right catheter. The CoA segment measured 3 mm; hence, pre-dilatation was done with an 8 mm × 20 cm peripheral balloon. Typically, balloon diameter for pre-dilatation should not exceed three times the diameter of narrowest segment. After that, a 16 × 44 mm uncovered stent [Zephyr stent (Sahajanand Laser Technology Limited, Gandhinagar, India)] mounted on an Atlas balloon (16 × 40 mm) was positioned across the CoA segment with 14 French Cooks sheath (Fig. 2) with hypotensive pacing rate of 180 beats per minute.
Fig. 2
A 16 × 44 mm uncovered stent (Zephyr) mounted on Atlas balloon being positioned across CoA segment
However, the stent slipped off the balloon during inflation and migrated proximally into the arch (Fig. 3).
Fig. 3
Slippage and proximal migration of the stent into the arch
As we tried to manipulate the system, the stent further migrated to the right brachiocephalic artery (Fig. 4).
Fig. 4
Migration of the stent further into the right brachiocephalic artery
The pigtail through the right radial route helped stabilize it and prevent further migration. We passed a low profile, shorter peripheral balloon (8 mm × 2 cm) through the stent and distal to it, inflated it, and pulled the entire system back (Fig. 5).
Fig. 5
Low-profile balloon (8 mm × 2 cm) distal to stent being inflated and entire system being pulled back
However, the lower edge of the stent got stuck at the tightest segment and was not coming down despite the pull. To overcome this, we dilated the CoA segment with a bigger 12 mm × 4 cm balloon (Fig. 6).
Fig. 6
CoA segment being dilated with bigger 12 mm × 4 cm balloon
After that we pulled down the entire system after inflating another balloon proximally, and this time, we were able to position the stent across the CoA segment. The same balloon was deflated and pulled into the stent, and the balloon stent assembly was inflated after proper positioning. Consequently, the stent was dilated with a larger 16-mm balloon and fully deployed across the CoA segment (Figs. 7, 8)—the gradient decreased to less than 5 mm Hg after stent deployment.
Fig. 7
Stent being dilated with larger 16-mm balloon and fully deployed across CoA segment
Fig. 8
Arch angiogram showing well-opened stent across the CoA segment
The access site was closed with Perclose ProGlide Suture-Mediated Closure System, and the patient was discharged after two days. A follow-up CT scan showed the stent in situ with no significant narrowing or other complications (Fig. 9).
Fig. 9
Follow-up CT image at 6 months showing well-expanded stent with no complications
Comments (0)