
Remember me
Hypertrophic cardiomyopathy (HCM) is a genetic cardiac disorder characterized by thickening of the heart muscle, notably the interventricular septum, which results in left ventricular outflow tract obstruction (LVOTO) and compromised cardiac function. HCM is among the leading causes of sudden cardiac death in young athletes, with an incidence of approximately 1 in 1,000 person-years [1]. While HCM primarily affects cardiac muscle, its association with coronary artery disease (CAD) presents a significant clinical challenge. Though the coexistence of CAD and HCM is infrequently documented, it markedly heightens the risk of myocardial ischemia and adverse cardiac events [2]. Multiple factors may contribute to the development of CAD in patients with HCM. Myocardial thickening can lead to reduced blood supply, increased myocardial oxygen demand, and heightened microvascular dysfunction [3]. Over time, these factors can precipitate ischemia, even in the absence of traditional coronary artery obstructions. Prompt diagnosis of CAD in HCM patients is therefore essential to optimize therapeutic strategies and improve both short-term and long-term clinical outcomes. Untreated ischemic episodes in these patients may further deteriorate cardiac function and elevate mortality risk [4].
This case report discusses a 40-year-old female patient with hypertrophic cardiomyopathy and coexistent coronary artery disease, who presented with worsening angina and dyspnea. Following coronary angiography, a two-stage treatment plan was developed, comprising percutaneous coronary intervention (PCI) followed by alcohol septal ablation. Due to the unavailability of the conventional OTW catheter during the procedure, an alternative 'block and delivery' technique was employed for the alcohol septal ablation, highlighting the procedural complexities of managing HCM in resource-limited settings such as Bangladesh.
Case Presentation A 40-year-old female presented with severe, non-radiating central chest pain and progressive dyspnea persisting for one day. Her chest pain was described as compressive and continuous, initially without radiation, and later accompanied by exertional dyspnea. She reported a history of similar exertional dyspnea over the past three years, with a recent exacerbation of symptoms. Her medical history was notable for hypertension, bronchial asthma, and four episodes of cardiac syncope occurring during moderate physical exertion over the last eight years.
On examination, the patient appeared dyspneic and was maintaining a propped-up position. Vital signs indicated a heart rate of 110 beats per minute, blood pressure of 110/60 mmHg, and a respiratory rate of 26 breaths per minute. Jugular venous pressure (JVP) was raised, measuring approximately 8 cm above the sternal angle.
Precordial examination revealed a forceful, sustained apex beat. The first heart sound (S1) was soft, while the second heart sound (S2) was normal. A pansystolic murmur was audible at the apex with radiation toward the axilla. Additionally, a non-radiating ejection systolic murmur was detected at the left parasternal edge. Respiratory examination indicated bilateral vesicular breath sounds with prolonged expiration, diffused rhonchi, and inspiratory crepitations in the lower zones of both lungs.
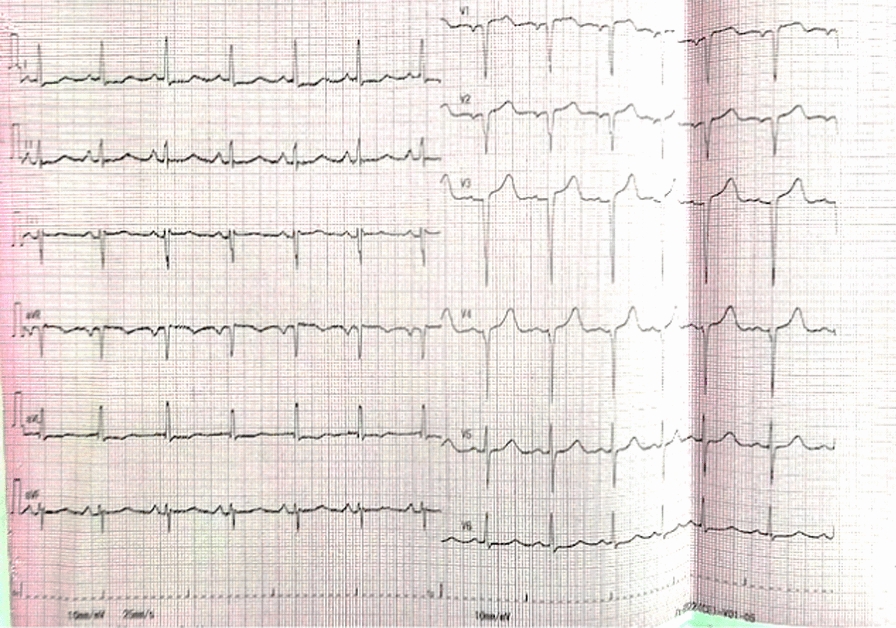
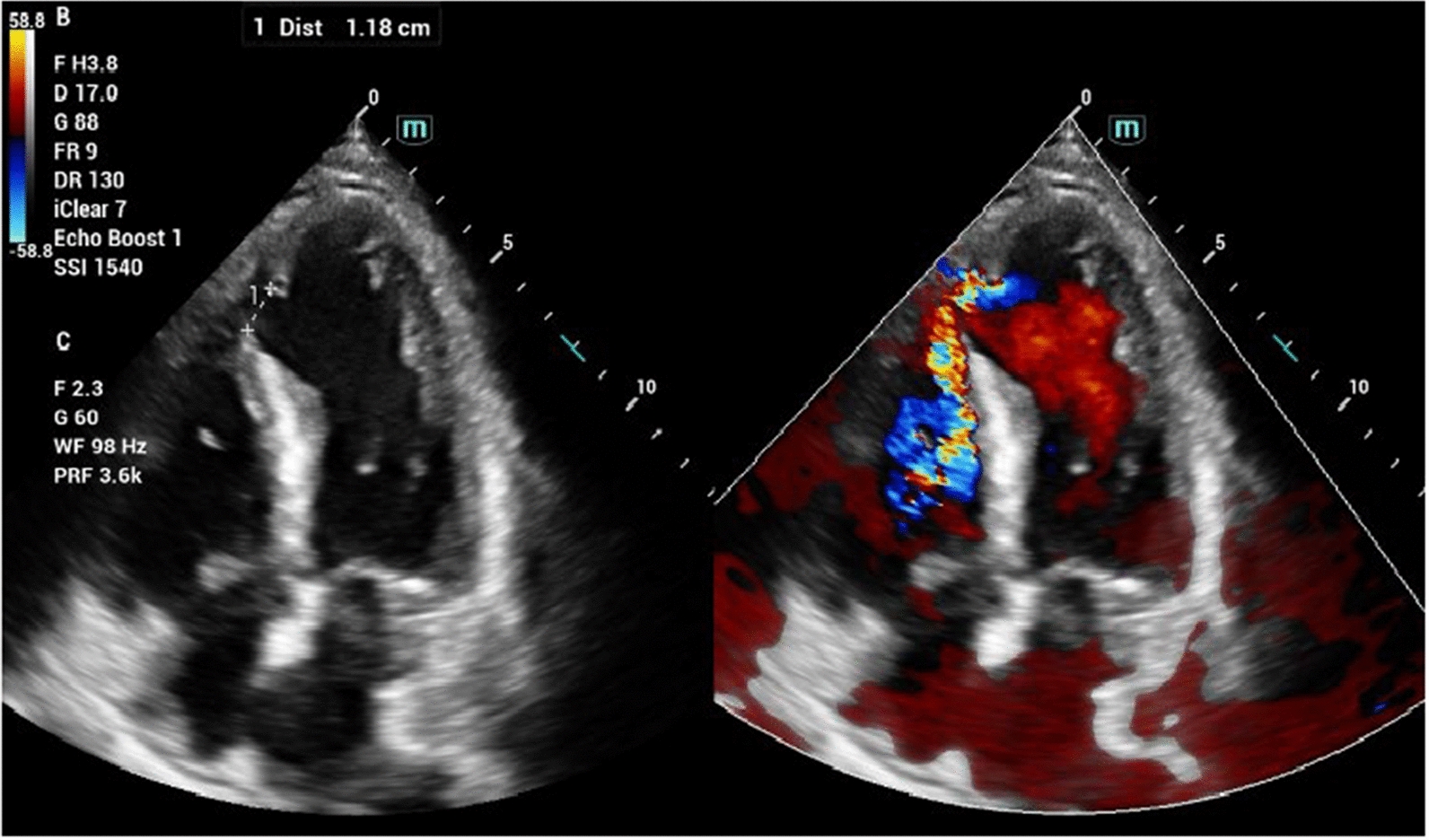
Initial laboratory tests revealed negative results for Troponin-I on two consecutive samples taken three hours apart, along with elevated NT-proBNP levels. The pre-procedure electrocardiogram demonstrated left atrial enlargement and poor R wave progression (Fig. 1). Chest X-ray findings were consistent with cardiomegaly. Transthoracic echocardiography confirmed hypertrophic cardiomyopathy (HCM) with systolic anterior motion of the anterior mitral leaflet, a severe left ventricular outflow tract (LVOT) gradient measuring 132 mmHg, and moderate mitral regurgitation. The septal thickness was measured at 20 mm (2.0 cm).
Fig. 1
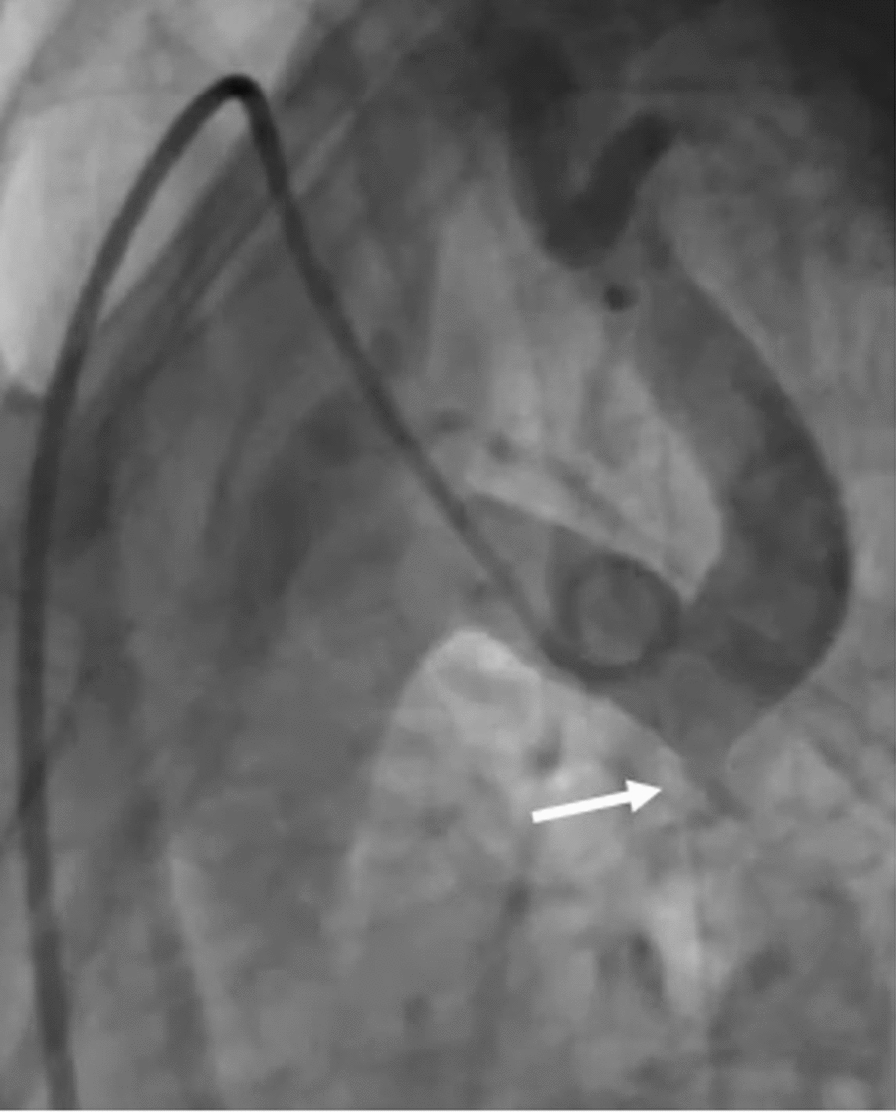
Considering the progressive symptomatology, coronary angiography was performed. The angiogram revealed 90% stenosis in the posterior descending artery (PDA) branch of the right coronary artery (RCA) and 40–50% stenosis in the proximal left anterior descending (LAD) artery, with a myocardial bridge identified in the mid-LAD.
Comments (0)