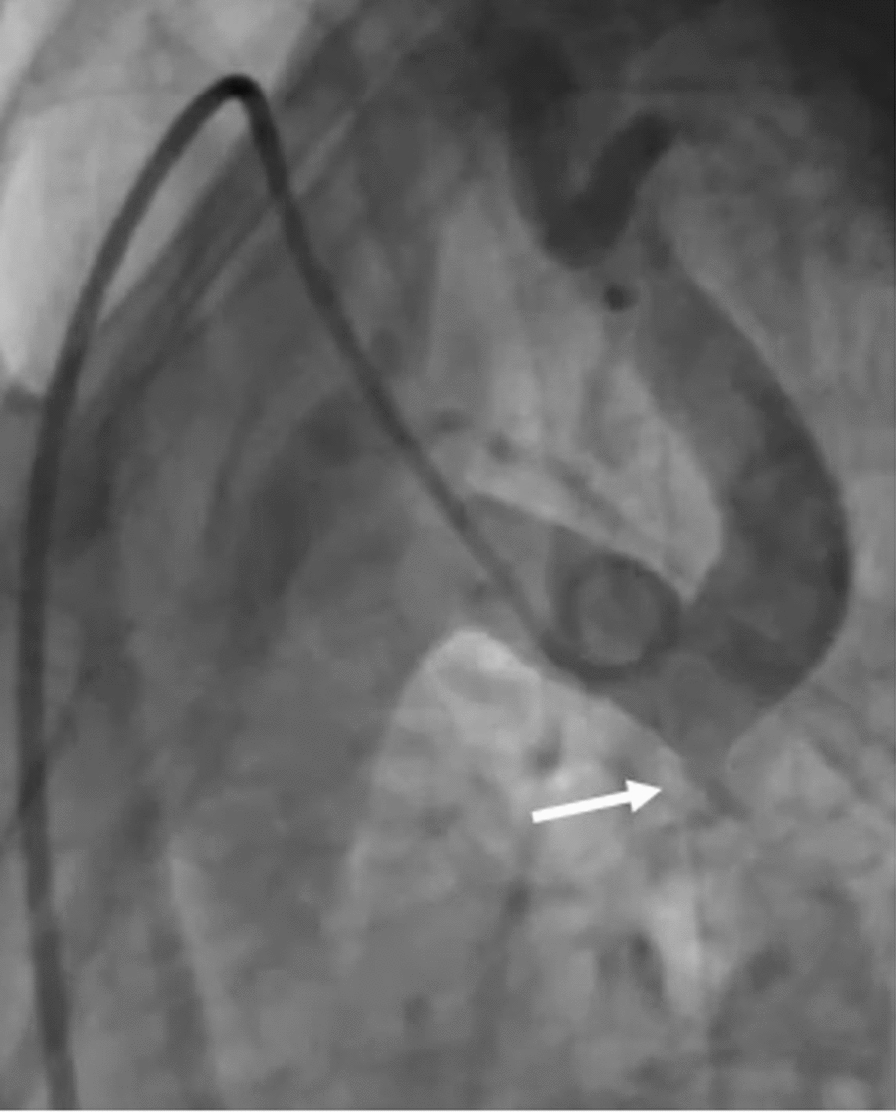
VSR is an infrequent but catastrophic complication of acute myocardial infarction, particularly following anterior STEMI [6, 7]. While its incidence has significantly decreased due to widespread adoption of revascularization strategies (from ∼1–2 to ∼0.25%), the risk of VSR remains in a subset of patients, especially those with delayed reperfusion or failed thrombolysis [6]. In the case we present, although rescue PCI was successfully performed with a DES in the LAD, the subsequent rupture of the interventricular septum complicated the clinical course (Fig. 1).
Our patient, who had a history of anterior STEMI, underwent rescue PCI after failed thrombolysis. Interestingly, in this case, the VSR manifested with acute heart failure and a pansystolic murmur at the apex four weeks after previous hospital discharge. VSR was confirmed at a secondary hospital, where the patient experienced worsening dyspnea and was referred to our tertiary hospital on day 36 with initial unstable hemodynamic status. Once a suspected VSR was confirmed by TTE, defect closure was advised [7, 8].
Surgical repair has long been the preferred treatment for VSR, as recommended by the guidelines of both the European Society of Cardiology and the American College of Cardiology [7,8,9]. However, this recommendation has not been supported by robust evidence due to the rarity of VSR in clinical practice and the limited data available from single-center experiences [10,11,12,13]. Therefore, the decision on closure strategies should tailored to the clinical condition.
Despite timely surgical intervention, a recent meta-analysis has reported in-hospital mortality rates for VSR of approximately 40%, with even higher rates in patients presenting with cardiogenic shock [12]. While immediate closure of VSR is advised, procedures performed within the first 24 h carry a mortality rate of 60% [10]. Surgeons are increasingly adopting a delayed surgical approach, particularly for hemodynamically stable patients. Mortality rates improve with delayed surgery—47% within the first week, 30% by the third week, and 10% for elective procedures performed after 21 days [10, 14]. Moreover, this surgical approach can be particularly challenging when the rupture occurs in the apical region, as in our case (Figs. 1 and 2). Apical VSR presents significant technical difficulties, including poor surgical visibility and limited access to the defect. Meanwhile, the patient was also maintained in a stable hemodynamic condition, even without pharmacological or mechanical circulatory support.
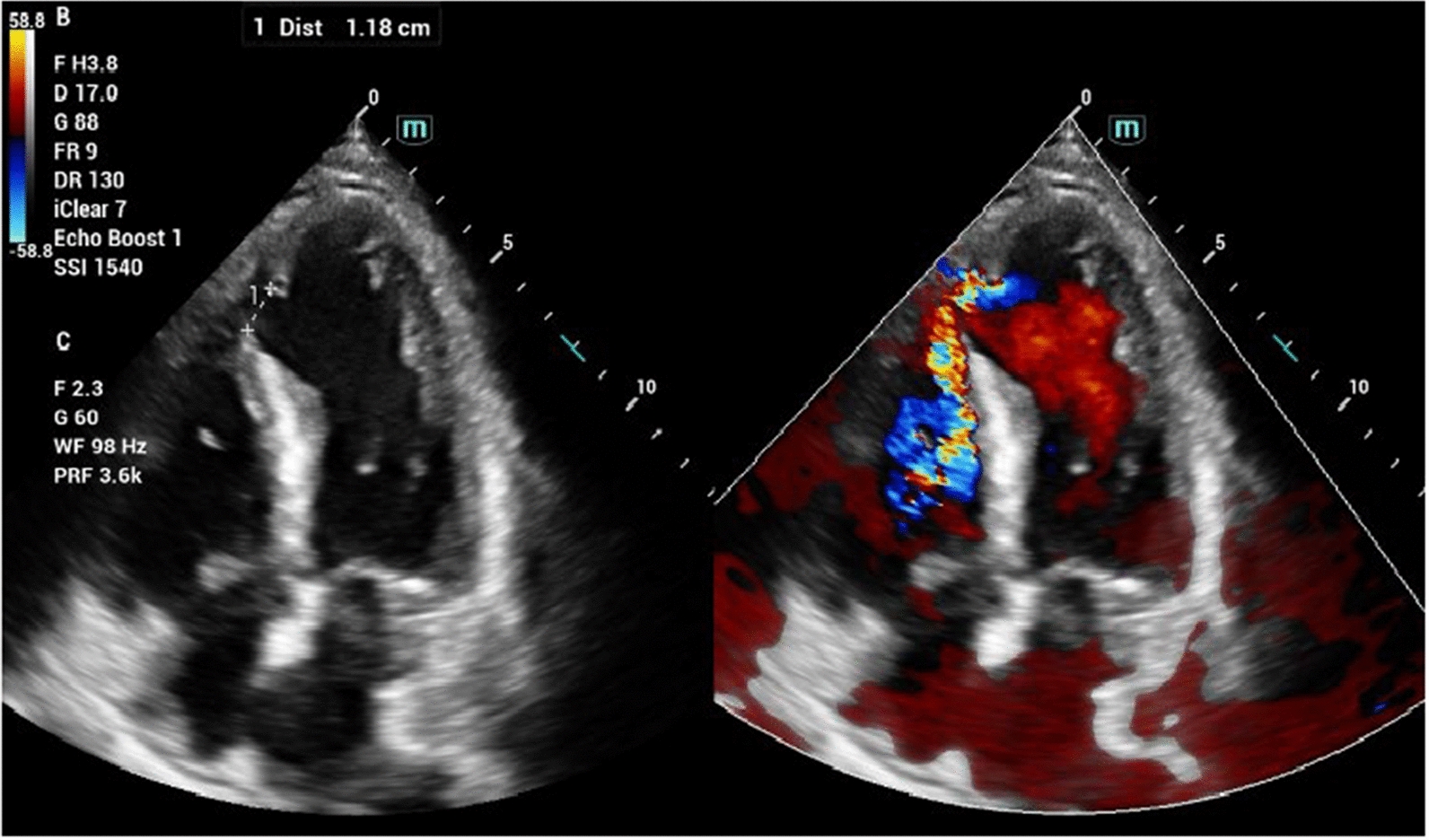
In recent years, percutaneous VSR closure has emerged as a promising alternative, particularly for patients at high risk of surgical closure, either as definitive therapy, bridge to surgery after stabilization, or correction of re-shunting due to patch leak [5]. For non-shock patients undergoing primary percutaneous closure around a median of 6.5 days post-VSR, mortality rates decrease to 38%, which is comparable to the surgical mortality observed in patients undergoing repair between 8 and 21 days (30%) [10, 15]. The current patient’s condition also favors percutaneous closure, as the VSR was identified 36 days after the onset of STEMI, which was subsequently adequately managed and stabilized. Literature, indeed, suggests that the occurrence of VSR typically peaks in the first 24 h or during the first week post-onset [8, 12]. Therefore, at the time of admission to our tertiary hospital (day 36), it was approximately 3–4 weeks since the presumed VSR occurrence (subacute VSR). With this timepoint, it was assumed that the infarct margins have evolved and stabilized, making device placement more optimal with a lower risk of defect enlargement, which could result in persisted post-procedural shunting [6, 16]. In line with our consideration, a series from China supported that percutaneous closure has a higher technical success rate when performed in a subacute setting compared to an acute one (97% vs. 78%). Moreover, the defect size observed from both echocardiography and ventriculography was less than 15 mm, which is considered in optimal range for percutaneous closure according to current recommendations [6, 17]. Diagnostic coronary angiography also revealed complete revascularization from the rescue PCI, showing only single vessel disease (in LAD). Thus, CABG was deemed unnecessary, and surgery was considered too invasive. The planned closure strategy, indeed, relies on several considerations, such as the complexity of the defect, the availability of appropriate device sizes, the speed of the procedure, the experience of the interventionist, the patient’s hemodynamic status, and the time from diagnosis to VSR occurrence [5]. This made the heart team’s decision to opt for percutaneous closure both logical and evidence-based.
The choice of vascular access is crucial in percutaneous VSR closure, with either the femoral or internal jugular vein being used for device delivery [8]. While the femoral vein is more commonly employed, the transjugular approach was considered more appropriate in this case. Drawing from experience with congenital muscular VSD, the internal jugular vein may be advantageous for treating muscular VSD closer to the apex [18]. Our interventionists considered that the jugular vein provided better angulation, enabling smoother catheter navigation from the right atrium to the right ventricle and through the VSR into the left ventricle. Thus, vascular access should be tailored to the specific clinical scenario.
Another challenge in this case was the selection of the closure device. Initially, we deployed muscular VSD occluder device. Nevertheless, the attempt was unsuccessful as too small to ensure adequate closure with subsequent device pull out. As a result, an ASD occluder, the largest device available in our center, was used to provide better closure (Figs. 3 and 4). Although not ideal, it effectively reduced the shunt with acceptable residual flow.

Comments (0)