Ischemic cardiomyopathy refers to reduced pumping ability of the heart due to myocardial changes resulting from ischemic process. In other words, ischemic cardiomyopathy shares similar risk factors with atherosclerosis. They can be divided into modifiable and non-modifiable risk factors. Modifiable risk factors include dyslipidemia, smoking, hypertension, diabetes mellitus, metabolic syndrome, and low physical activity, while non-modifiable risk factors include old age, male sex, and genetics. They all contribute to the pathophysiology of atherosclerosis, which includes endothelial dysfunction, oxidative stress, and lipid accumulation. In addition to atherosclerosis, remodeling processes also contribute to ischemic cardiomyopathy. Risk factors for myocardial remodeling include high hemodynamic stress, neurohormonal activation, and oxidative stress [7]. These reasons may explain the finding in this study that the percentage of risk factors for atherosclerosis and myocardial remodeling was high.
The median sST2 level in this study was 5.6 ng/mL (IQR: 2.0–11.5 ng/mL). A previous study by Broch et al. evaluated sST2 level in ischemic heart failure. The sample population in this study was patients with ischemic heart failure with NYHA class II-IV, LVEF < 40%, and age > 60 years. In the study by Broch et al., out of a total of 1449 patients, the median sST2 level was 17.8 (0.2–400.0) ng/mL [8], while the study by Dimitropoulos evaluated sST2 levels in 143 HFrEF patients with ischemic etiology and found that the mean sST2 was 15.8 ng/mL [9]. This indicates that sST2 levels in this study were much lower than in the ischemic cardiomyopathy population in the other studies. The lower sST2 result compared to other studies may be due to the lower severity of our study population, as 90% of the population classified as NYHA II. The population in this study came from a heart failure clinic where these patients had been receiving guideline-directed medical therapy (GDMT), which was very concerned that although many EFs were low, they could functionally return to NYHA functional class II. In the 2014, the pro-BNP outpatient chronic heart failure therapy (PROTECT) study by Gaggin et al. evaluated the ability of sST2 to identify the risk of left ventricular remodeling in outpatients with low ejection fraction heart failure. This study found that sST2 levels < 35 ng/L had a lower probability of end-diastolic volume index in the first year compared to the group with sST2 levels > 35 ng/mL [10].
Suppression of tumorigenicity 2 is a biomarker of myocardial stress. Weinberg et al. found that transcription of the ST2 gene, especially sST2, was significantly increased in myocytes and cardiac fibroblasts from mice subjected to mechanical stress or myocardial injury in conditions such as myocardial infarction. These results were further confirmed by several in vitro studies reporting similar results [11,12,13]. Soluble ST2 (sST2) also plays a role in myocardial fibrosis through pathways involving the extracellular matrix. The study by Martinez et al. showed that sST2 was able to stimulate extracellular matrix synthesis by increasing the synthesis of collagen and fibronectin through profibrotic molecules such as TGF-β and connective tissue growth factor (CTGF) [14]. A study conducted by Daniel et al. in 2010 stated that patients with high sST2 levels due to acute myocardial infarction had more significant changes in heart shape than patients with low sST2 levels. Studies suggest that sST2 can be used as a prognostic biomarker to detect heart conditions [15]. Thus, it can be concluded that the heart condition in this study population is better than other studies. This is supported by the finding that the percentage of patients with NYHA class II in this study was higher than in previous studies [90% (this study) versus 68% (Dimitropoulos et al.) and 32.2% (Broch et al.)]. The study by Broch et al. and Dimitropoulos et al. included more patients with NYHA class III and IV than this study [8, 9], but further studies are needed to confirm the exact cause of the low sST2 values in this study. It should be noted that sST2 levels were reported to be unaffected or unrelated to age, body mass index, serum creatinine, and smoking as well as other biomarkers such as CRP, galectin-3, MMP 9, TIMP, and brain natriuretic peptide (BNP). Weinberg et al. in 2013 also stated that sST2 levels did not differ significantly with age, race, and body mass index. Serum sST2 levels were also not affected by the time of collection because the intra-individual biological variation of sST2 was only 11%. Meanwhile, the inter-individual variation of sST2 levels was reported to be 46% with a reference value of 30 [13].
In this study, the median MMI was found to be 34.0% (IQR: 23.0–42.3%). Ivanov et al. performed a screening of DM ECG examination and assessed MMI. In a total of 537,830 people screened in Russia, MMI values were found to be weakly related to gender and age. The study divided the MMI ranges into normal (< 15%), borderline (15–21%), and pathological (> 21%). Similar to this study, we found no correlation between MMI with age and sex in a small number of subjects (n = 30). Study by Ivanov et al. found that the prevalence of patients with borderline MMI increased at age 35 years and the prevalence of pathological MMI increased at age 55 years [16]. There are limited studies on MMI measurement in the general population. To best of our knowledge, there have been no studies with English publications evaluating the value of MMI in patients with ischemic cardiomyopathy. However, a study conducted by Bulgakova et al. evaluated the MMI value in patients with acute coronary syndromes. The median MMI value was 24% [17]. Another study evaluated the MMI in acutely ill patients. The study by Kellet et al. found that the mean MMI of acutely ill patients was 23.4%. Kellet et al. also found that MMI was associated with worsening in acutely ill patients [6]. The MMI in these studies was much lower than in this study, because the study population was patients with ischemic cardiomyopathy, who certainly have a higher chronic myocardial remodeling than acutely ill patients and patients with acute coronary syndromes.
The results of correlation analysis using Spearman's rank showed that there was a significant correlation with moderate power between the myocardial micro-alternation index and soluble ST2 (r = 0.583, p < 0.05). To the best of our knowledge, there has been no study on association between sST2 and MMI in patients with ischemic cardiomyopathy. The association of structural and electrical remodeling in ischemic cardiomyopathy may give clue for better early treatment in such patients. Cardiac remodeling due to fibrosis can be detected by sST2 because of the mechanism described earlier. The process of fibrosis in the heart will affect the flow of electricity in the myocardium, causing arrhythmias. The study by Atabekov et al. found a significant association between sST2 and ventricular arrhythmias in ACS patients with reduced LVEF [18]. Another study by Lashkul et al. found a significant association between sST2 and Left Atrial Volume Index (LAVI) in patients with ischemic cardiomyopathy [19]. It has been known that LAVI was also associated with atrial fibrillation. Another study by Mashlovskyi et al. showed that in NSTEMI patients, higher sST2 levels were associated with the development of ventricular tachycardia and ST segment depression [20]. A study by Skali et al. in 2016 through the Multicenter Automated Defibrillator Implantation Trial (MADIT) evaluated the risk of ventricular arrhythmias in relation to sST2 level in cardiomyopathic patients receiving cardiac resynchronization therapy defibrillator (CRT-D) [21]. sST2 can predict mortality and the incidence of ventricular arrhythmias in patients indicated for CRT-D placement due to ischemic and non-ischemic heart failure. The study also found that serially elevated sST2 levels were associated with a higher risk of ventricular arrhythmias and death or the occurrence of ventricular arrhythmias. In addition, subjects with lower baseline sST2 may benefit more from CRT-D therapy than subjects with higher sST2 [21]. These studies have shown that sST2 is associated with the development of arrhythmias in patients with ischemic heart disease, including ischemic cardiomyopathy. Another study by Broch, et al. in 2016 stated that there was an independent association between sST2 and ventricular arrhythmias in patients with arrhythmogenic right ventricular cardiomyopathy (ARVC). In addition, sST2 also exhibited right-sided heart failure and is independently associated with potentially fatal arrhythmias in this population [8].
Studies on mice by Weinberg et al. and Kakkar et al. have shown that ST2 is associated with myocardial fibrosis and hypertrophy through its interaction with IL-33. Myocardial hypertrophy and fibrosis could reduce cardiac compliance and decrease the diastolic relaxation properties of the heart chambers, leading to disrupted filling of the heart. These conditions indicated that ST2 expression was associated with cell damage and cardiac remodeling which was the pathophysiological basis for cardiomyopathy [13]. In addition to structural remodeling, electrical remodeling also took place in ischemic cardiomyopathy. Hegyi et al. in 2018 conducted a trial by embolization of the porcine anterior descending coronary artery and evaluated the resulting electrophysiological changes at 5 months after infarction. Myocytes in the border zone of the infarct had a shortened action potential duration, whereas myocytes far from the infarct experienced a lengthening of the action potential. These findings suggest that heterogeneous remodeling of the action potential due to ischemia causes a dispersion of action potential duration between the infarct border zone and the remote infarct zone which may be a substrate for arrhythmias. Not only action potentials, but also other heterogeneous electrophysiological remodeling existed between the borderline zone and the far infarct zone such as peak potential, resting membrane potential, maximal upstroke velocity, and maximal rate of repolarization. The finding of their study indicates that ischemic heart failure causes chronic electrical remodeling of the heart. Electrical remodeling contributes to the difference in inflow and outflow of various ions between cardiac cells and ultimately increases the risk of arrhythmia development. However, electrical remodeling in ischemic heart failure is often not detected by ECG, so other modalities that can detect micro-electrical changes in the heart, such as MMI, are needed [22].
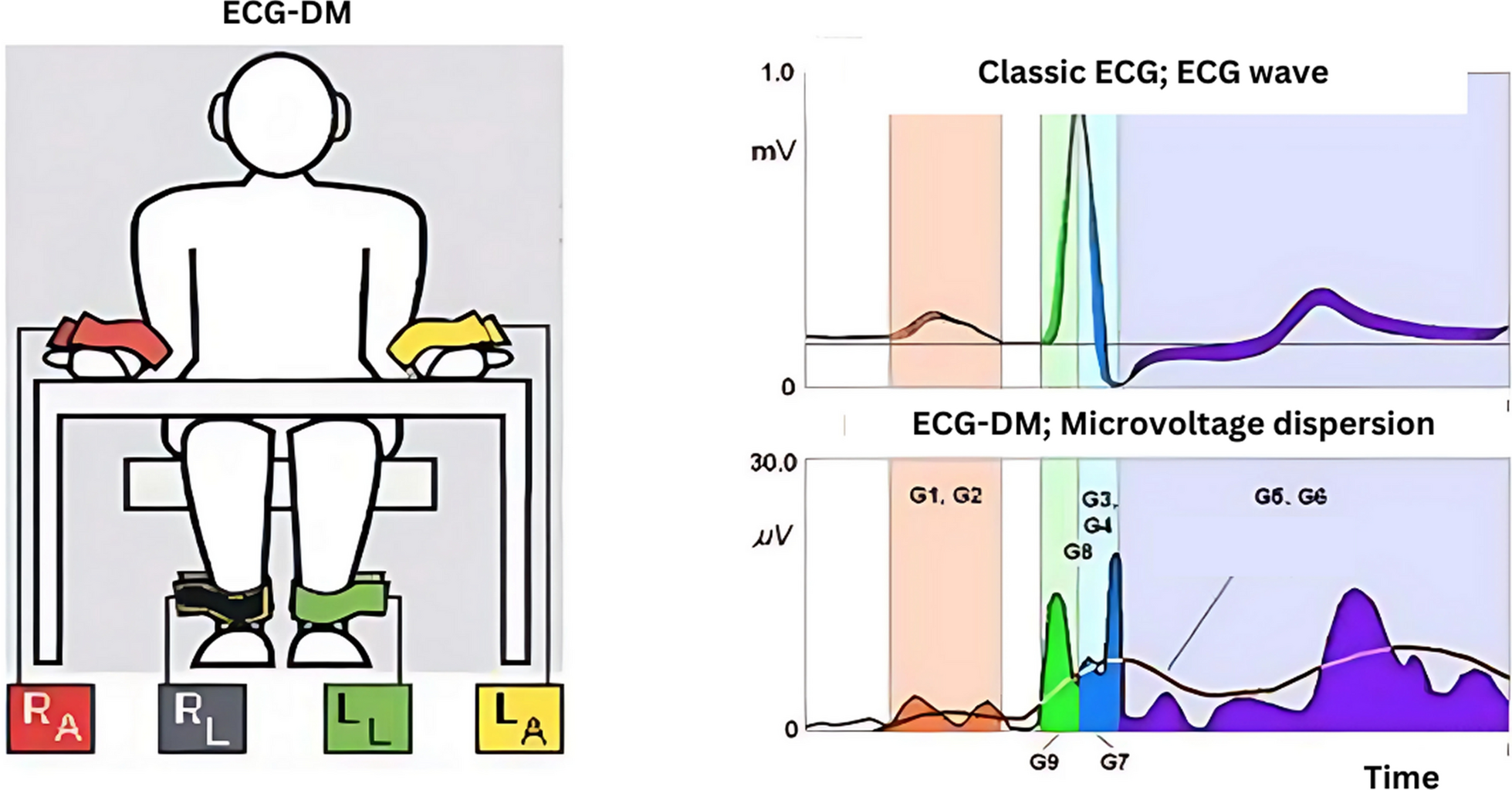
The DM ECG method can be referred to as the ECG micro-change recording method. This method is a relatively new non-invasive way of looking at myocardial electrical instability. The amplitude of the micro-changes can be twice as small as the amplitude of the conventional ECG waves.18 One of the assessments in the DM ECG is the MMI. MMI, as previously described, reflects abnormalities in the myocardium at the metabolic rate, which may include ischemia and other causes by detecting micro-alterations in the electrical properties of the heart [6]. In ischemic cardiomyopathy, both structural and electrical remodeling occur. Structural remodeling is characterized by an increase in sST2, whereas electrical remodeling is characterized by changes in MMI. This study found that MMI was significantly correlated with sST2, indicating that there was a correlation between structural and electrical remodeling in ischemic cardiomyopathy. The MMI examination has the advantage of being easy to use and the results obtained are already in the form of numbers, providing a more objective interpretation than other ECG parameters that are operator dependent. The finding of this study may provide evidence for the use of MMI as an effective modality in the risk stratification of patients with ischemic cardiomyopathy. Further studies with larger sample sizes are needed to assess the feasibility of MMI as a risk stratification modality for patients with ischemic cardiomyopathy.

Comments (0)