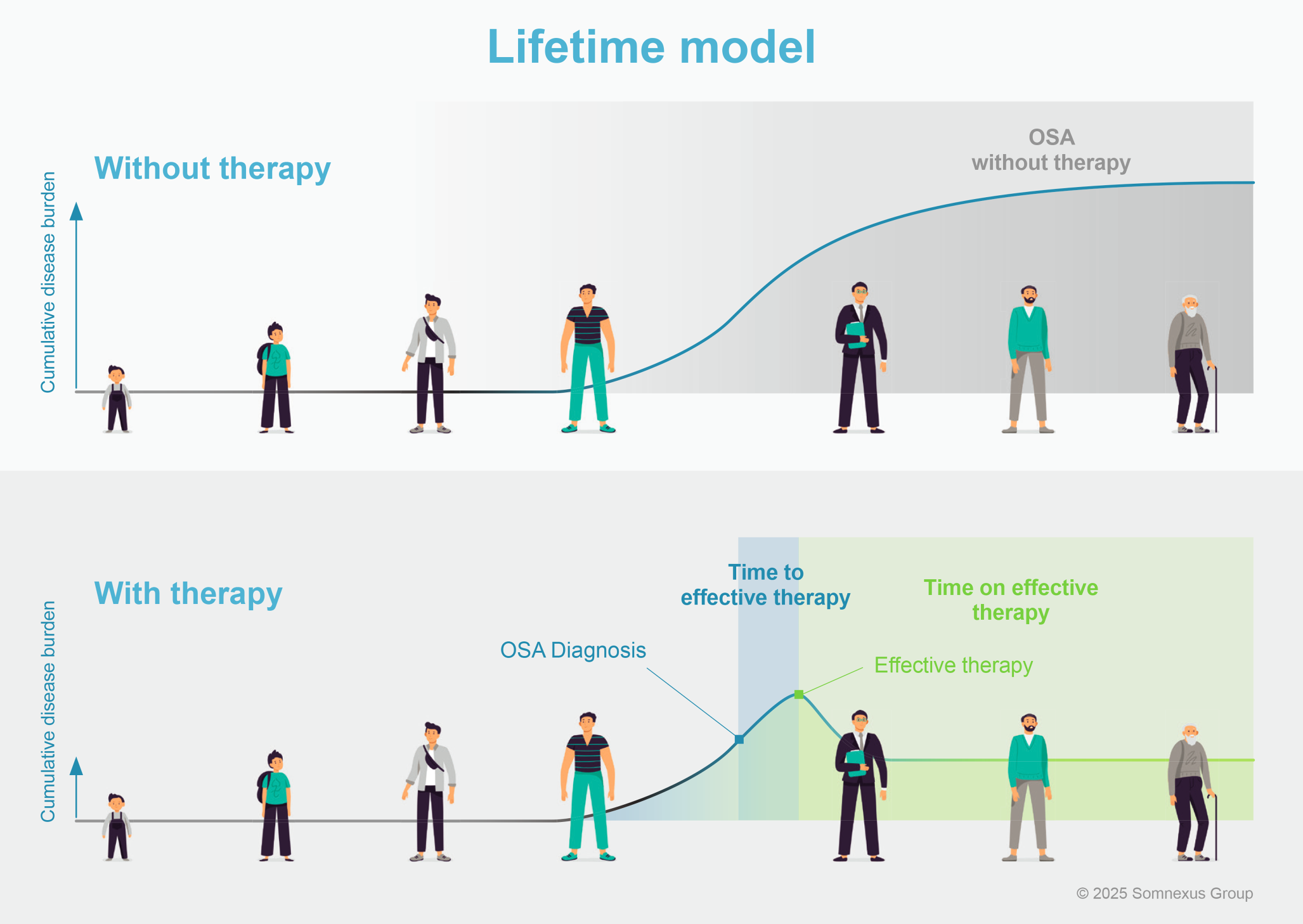
In principle, there is limited literature on the validation of different concepts of long-term care of OSA patients with different therapeutic modalities [3, 8, 21]. In particular, there is a lack of studies that go beyond the apnea–hypopnea index and device use to define effective therapy [3, 8, 21], patient satisfaction, and the effects on sleep quality and symptoms. At present, we are also not aware of any studies that have compared the time to effective therapy or the time on effective therapy between different forms of care that consider all available therapy modalities.
The S‑O‑S concept presented here addresses aspects that have so far received little attention in the long-term care of OSA patients. The S‑O‑S concept will therefore be validated step by step. Initially, a qualitative test phase with an approximate enrollment of 200 OSA patients will be carried out to investigate acceptance and feasibility from both the patient and physician perspective. Important endpoints of the first test phase are the completeness of the S-O-S questionnaire, the proportion of patients on effective therapy, the need for optimization, and the need to change therapy at the timepoints 1–6 months and 9–15 months. In addition, the intervals at which the optimization cycles actually take place in clinical routine and how much time is required for the treatment changes will be evaluated.
In the second phase, the current standard long-term care will be compared with care based on the principles of the S‑O‑S concept in approximately 2000 OSA patients. In this study, the proportion of patients on effective therapy after 1 and 2 years and the time on effective therapy within the first and second year will be compared between the care models. Furthermore, the proportion of patients on specific OSA therapies will be compared.
Various definitions of “effective OSA therapy” will be used, as it cannot be assumed that the components of patient satisfaction, reduction in apnea burden (apnea–hypopnea index taking into account the time of use), change in sleep quality, and OSA-dependent complaints are always assessed and documented in clinical routine for all forms of care. Exploratory analyses of interest will determine whether the various components (patient satisfaction, improvement in sleep quality, etc.) of effective OSA therapy have an impact on target parameters relevant to patients, such as quality of life or prognosis.
Structural aspects
As sleep medicine happens across multiple environments and sectors, intersectoral collaboration is required. Interdisciplinary collaboration is also necessary, as both sleep medicine and the ability to carry out outpatient polygraphy (“BuB certification”) are located in different specialist areas. This must be organized locally due to the different regional circumstances. Sleep medicine quality circles would be one possibility for this. To date, there has been no remuneration for treatment follow-up in the statutory health insurance system outside of technical examinations (polygraphy/polysomnography). This problem must be solved in terms of health policy. Due to the long-term therapy management and the risk factors to be optimized in parallel, the introduction of a disease management program (DMP) for sleep apnea would also make sense.





Comments (0)