
Remember me

The safety profile of melatonin has been extensively documented in both animal and human studies. Short-term use of melatonin, even at high pharmacological doses, has been consistently shown to be well tolerated, with no serious adverse events reported. Similarly, randomised clinical trials have shown that long-term administration of melatonin is only associated with mild adverse effects that are comparable in frequency and severity to those reported with a placebo [17, 19]. Although large-scale randomised clinical trials that evaluate chronic high-dose melatonin administration remain limited, existing studies confirm its low toxicity and favourable safety profile [18, 20]. In this regard, melatonin has been administered in a wide range of daily doses in humans, ranging from 0.1 mg to 3 g per day (summarised in Supplementary Table S1), with no evidence of serious adverse effects [17,18,19]. Oral doses of up to 0.3 mg maintain plasma melatonin levels within the endogenous range [26], serving as the threshold between high physiological and low pharmacological doses. In Europe, melatonin is available as a dietary supplement at doses below 2 mg, which can increase endogenous levels up to tenfold without reported adverse effects [27].
Regarding high-dose trials, a pilot study in three patients with amyotrophic lateral sclerosis (ALS) who received oral doses of 30–60 mg/day for 13 months reported no intolerance, side effects, fatigue or changes in biochemical markers [28]. A larger trial involving 31 patients with ALS treated with 300 mg/day of rectal melatonin for 2 years found that serum melatonin levels remained stable over time, indicating that its metabolism was not altered. Routine laboratory tests showed no significant abnormalities [29]. Furthermore, a randomised, double-blind, placebo-controlled trial conducted in 24 male athletes receiving 100 mg/day of oral melatonin or a placebo revealed no evidence of hypertransaminasemia, as demonstrated by normal plasma levels of AST and ALT that remained unchanged throughout the 4-week treatment. In fact, LDH levels decreased significantly after melatonin treatment, with no changes observed in the placebo group [30]. In addition, in a placebo-controlled study conducted in 54 male patients, who had been subjected to varicocelectomy, receiving 400 mg/day of oral melatonin or placebo for 3 months, no adverse effects were reported [31]. Studies in healthy women have also confirmed the safety of high-dose melatonin. In a trial, 12 women who received 300 mg/day for 4 months did not experience adverse events [32]. A double-blind, randomised, placebo-controlled trial in 50 patients (68,18% women) with type 2 diabetes mellitus (T2DM), who ingested 250 mg of melatonin once a day for 8 weeks concluded that melatonin supplementation may be effective in controlling clinical events related to T2DM without reporting adverse events or side effects [33]. In addition, a case report described an improvement in the EDSS score in a woman patient with PP-MS taking 300 mg/day for 4 years, with no reported adverse events [22]. A 4 weeks ingestion of 1 g/day melatonin (4 doses of 250 mg throughout the day) in five human subjects with hyperpigmented skin (4 of them were women) did not show any sign of toxicity related to the eyes, liver, kidneys and bone marrow, beyond increased drowsiness [34]. A randomized controlled trial in 20 women with amenorrhea treated with 3 g/day of melatonin combined with myo-inositol for 6 months found no side effects compared with the control group [35].
Studies also indicate that daily administration of melatonin at low-to-moderate pharmacological doses (20–100 mg) does not cause significant side effects beyond mild sleep disturbances and fatigue. Regarding MS, a recent systematic review has shown that melatonin supplementation (ranging from 2 to 25 mg/day in treatments from 2 weeks up to 6 months) exerts benefits in oxidative stress, inflammatory status and MS symptoms, such as fatigue, without significant safety issues [36]. In particular, in a double-bind, randomised, placebo-controlled trial conducted in 36 patients with RR-MS (26 women) receiving 25 mg/day of oral melatonin or placebo for 6 months, no significant differences were observed in side effects rates compared with placebo [37].
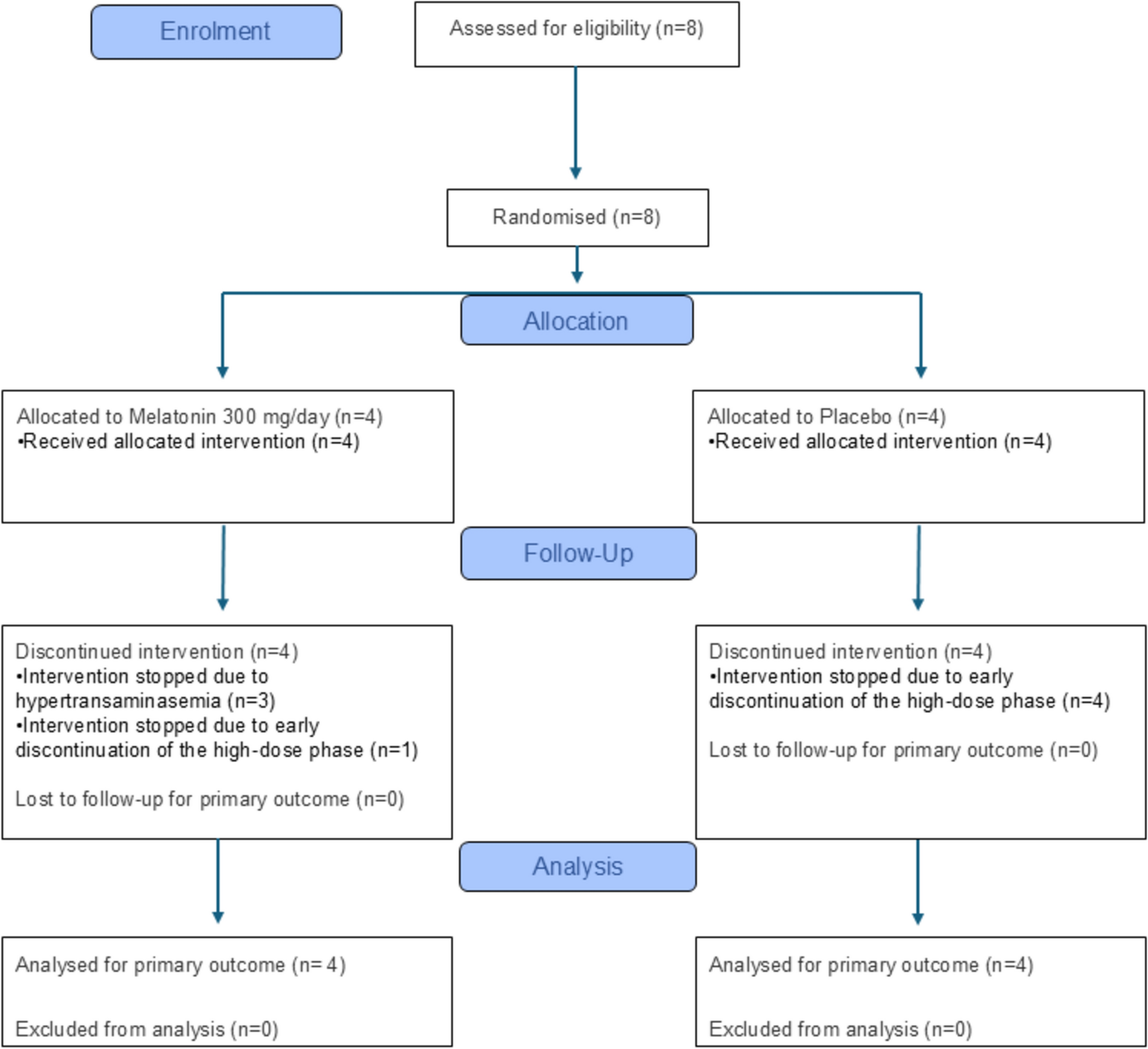
Despite the well-documented safety profile of melatonin, the MELATOMS-1 trial was temporally interrupted and unblinded due to three cases of hypertransaminasemia, all of which occurred in the melatonin group. Given the extensive literature supporting the hepatoprotective role of melatonin [38, 39], this unexpected finding led to a further analysis of patient characteristics and hepatic metabolism in the context of polymedication to explore the possible causal mechanisms underlying the observed increase in transaminase levels.
Hepatotoxicity is an important reason why drugs in development may not continue. Because all participants in the MELATOMS-1 trial received ocrelizumab as background therapy, its potential contribution to the observed hepatotoxicity was carefully considered. Ocrelizumab, a humanized anti-CD20 monoclonal antibody, has a generally favourable liver safety profile. Large clinical trials and long-term studies have not demonstrated drug-induced hepatotoxicity or clinically relevant elevations in liver enzymes in most patients with multiple sclerosis [40, 41]. Most hepatic adverse events are mild and transient [42, 43], while rare cases of acute or autoimmune hepatitis and fulminant liver failure appear to be idiosyncratic and unpredictable [44, 45]. The main liver risk associated with ocrelizumab is hepatitis B virus reactivation [46, 47]; however, all participants in this study were screened negative for HBV infection before enrolment, and no viral reactivation occurred during follow-up. Therefore, ocrelizumab is unlikely to explain the transaminase elevations observed in participants treated with melatonin.
Identifying the exact cause of DILI is often complex [48], but in this study, a temporal relationship with melatonin treatment appears plausible, as hypertransaminasemia occurred exclusively in the melatonin group, and liver enzyme levels improved after discontinuation of melatonin. In addition, case 2 experienced a recurrence of hypertransaminasemia after melatonin reintroduction. However, this patient experienced a sharp decrease in transaminase levels just 1 day after discontinuing melatonin (ALT: 75%, AST: 60%, GGT: 25%), suggesting that other factors, such as a viral infection or gallstone disease, may have contributed.
Unfortunately, no complementary tests were performed to confirm this hypothesis. According to the severity rating scale of the International DILI Expert Working Group, only case 2 was classified as grade 2 (moderate toxicity), while the other two cases were grade 1 (mild). The Roussel Uclaf Causality Assessment Method (RUCAM) score [49] was not calculated due to its limitations in the context of clinical trials.
The three patients who developed hypertransaminasemia were women, a factor linked to an increased susceptibility to drug-induced hepatotoxicity. Epidemiological studies suggest that women have a greater predisposition to develop DILI and acute liver failure than men [50]. This sex-based vulnerability is likely related to differences in drug bioavailability, metabolism and excretion, as well as hormonal influences on liver enzyme activity [51]. Interestingly, the only patient in the melatonin group who did not develop hypertransaminasemia was a man, despite receiving the same dose of melatonin and being the longest-treated participant (14 months of uninterrupted melatonin intake). This observation further supports the hypothesis that sex differences may play a role in susceptibility to hypertransaminasemia.
Another common feature observed in affected patients was a mild increase in CRP levels, which occurred concomitantly with hypertransaminasemia in all three cases treated with melatonin. This consistent temporal association suggests that CRP elevation most likely reflected a secondary acute-phase response to hepatic inflammation rather than a marker of systemic disease activity. Although elevated CRP levels are rare in clinically stable primary progressive multiple sclerosis (PP-MS) [52], mild and transient increases have been reported in association with tissue injury or intercurrent inflammation [53, 54]. In our study, CRP levels remained below 13 mg/L and normalised after discontinuation of melatonin, paralleling the resolution of liver enzyme abnormalities. All participants received ocrelizumab, which is not known to induce liver inflammation or acute-phase responses, and the placebo subject who showed a mild CRP increase (7.1 mg/L) did not show any biochemical or clinical evidence of hepatotoxicity. Melatonin and placebo capsules contained identical excipients, excluding a formulation-related effect. In this regard, the excipient contained in each capsule was microcrystalline cellulose, colloidal silicon dioxide and magnesium stearate. There is no published evidence linking the administration of any of these components, commonly used as components of formulations in clinical trials, with elevated CRP levels or liver injury, when administered alone or in combination with other drugs [55,56,57]. Altogether, these findings suggest that CRP elevation represented a non-specific acute-phase reaction secondary to mild hepatocellular injury, rather than a direct consequence of melatonin or an exacerbation of PP-MS. However, the lack of CRP measurements at certain time points prevented us from drawing definitive conclusions.
A key finding in this study is that all affected patients were taking multiple concomitant medications that share liver metabolic pathways with melatonin, suggesting a possible mechanism of metabolic overload or enzymatic inhibition. The liver plays a central role in drug metabolism, regulating the clearance of both xenobiotics and certain endogenous molecules. Hepatic metabolism is largely mediated by the cytochrome P450 (CYP) enzyme system, which consists of a wide variety of isoforms, with CYP 1A2, 2D6, 2C9, 2C19 and 3A4 being responsible for 60% of drug metabolism [58]. The main catabolic pathway of melatonin involves the hepatic CYP1A2 enzymatic isoform, which catalyses the conversion of melatonin to 6-hydroxymelatonin (6-OHM) and, to a lesser extent, to N-acetylserotonin (NAS) by O-demethylation (Fig. 3) [59]. These metabolites are subsequently conjugated with sulfate or glucuronide through sulfotransferases (SULTs) and UDP-glucuronosyltransferases (UGTs), and are ultimately excreted in the urine [60]. Furthermore, other CYP isoforms, such as CYP2C9, CYP1C19 and CYP1A1, are also involved in melatonin catabolism, although their activity is considered minor [61].
Fig. 3 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Diagram of the main pathways involved in the hepatic catabolism of melatonin. The major process of MLT breakdown occurs in the liver via the hepatic enzyme CYP1A2, which performs 6-hydroxylation to convert melatonin to 6-hydroxymelatonin and O-demethylation to produce N-acetylserotonin within hepatocytes. Subsequently, both 6-hydroxymelatonin and N-acetylserotonin undergo conjugation with sulfate or glucuronide by sulfotransferases and UDP-glucuronosyltransferases, respectively, and are ultimately eliminated from the body through the urine. In addition, other CYP isoforms, such as CYP2C9, CYP1C19 and CYP1A1, are involved in melatonin catabolism, although their contribution is minimal. CYP, cytochrome P450; UGT, UDP-glucuronosyltransferase; SULT, sulfotransferase
In the MELATOMS-1 clinical trial, melatonin was administered at a high pharmacological dose to ensure its maximum concentration in the central nervous system (CNS) and enhance its potential neuroprotective effects. Many of the drugs taken concomitantly by study participants share the same metabolic pathways as melatonin, including CYP isoforms, SULTs and UGTs. The enzymatic activity of CYPs can be inhibited by certain drugs and/or overwhelmed by competitive substrates, leading to drug accumulation and potential toxicity. This raises the possibility that melatonin may have saturated the enzymatic capacity of CYPs (1A2, 2C19, 2C9 and/or 1A1) as well as the conjugation pathways of SULTs (1A1, 1A2, 1A3, 1B1 or 1E1) [62] and UGTs (UGT1A9 and UGT1A10) [63]. Such saturation could result in the accumulation of hepatotoxic substrates, particularly at inappropriate doses [64].
Previous studies have established a dose-independent association between drugs metabolised by CYP enzymes and an increased risk of DILI [65]. Furthermore, research has shown that drugs inhibiting non-CYP enzymes, such as UGTs, are significantly associated with a higher risk of hepatotoxicity [66]. Since UGTs are involved in the conjugation of endogenous molecules such as bilirubin, bile acids, serotonin, steroid hormones and eicosanoids [67], reduced UGT activity can alter the normal metabolic clearance of these substances, leading to bioaccumulation and prolonged biological effects.
Figure 4 summarises the metabolic pathways involved in the hepatic clearance of medications taken by patients receiving melatonin or placebo. In case 1, the patient was taking acetaminophen, metamizole and dalfampridine, in addition to melatonin. Acetaminophen is excreted primarily in urine as non-toxic glucuronidated and sulfated metabolites [68], but a small fraction undergoes oxidation mediated by CYP (2E1 and to a lesser extent by 1A2 and 3A4), generating N-acetyl-p-benzoquinone imine (NAPQI), a highly reactive metabolite detoxified by conjugation with reduced glutathione (GSH) [69]. At high doses of acetaminophen, the glucuronidation and sulfation pathways become saturated, increasing CYP metabolism and NAPQI production [70]. If excess NAPQI accumulates beyond the available detoxification capacity of GSH, liver necrosis can occur. Although the acetaminophen dose in this case was low, the presence of elevated melatonin metabolites (6-OHM and NAS) may have competed for the glucuronidation and sulfation pathways, reducing acetaminophen clearance and facilitating NAPQI accumulation and liver injury. In addition, metamizole, a known CYP3A4 inducer, may have further increased NAPQI production, compounding the risk of hepatotoxicity (Fig. 5) [71].
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Enzymes involved in the liver metabolism of drugs taken by patients. The CYP450 isoforms involved and not involved in melatonin (MLT) hepatic metabolism are listed in the left and right columns, respectively. The LiverTox index of each drug is indicated in brackets [64]. Drugs that do not undergo liver catabolism have not been identified. Within phase I reactions, the main CYP isoforms used by each drug are coloured red, and the isoforms used in a minority way are coloured blue. For phase II enzymes, we used the green colour [69]. CYP, cytochrome P450; n/a: not available; UGT, UDP-glucuronosyltransferase; SULT, sulfotransferase
Fig. 5 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Hypothetical scheme of possible drug interactions that would have occurred in case 1. High doses of melatonin would saturate the enzymes responsible for hepatic conjugation with glucuronide and sulfate, UDP-glucuronosyltransferases and sulfotransferases, compromising the elimination of acetaminophen and thus causing an accumulation of NAPQI. CYP, cytochrome P450; NAPQI, N-acetyl-p-benzoquinone imine; UGT, UDP-glucuronosyltransferase; SULT, sulfotransferase
In case 2, the patient was taking dalfampridine, omeprazole, ibuprofen and sertraline, all of which interact with CYP enzymes. Omeprazole and ibuprofen are classified by LiverTox as categories B and A, respectively [64]. LiverTox is a widely used reference tool for evaluating hepatotoxic potential. It is an expert-reviewed online database created by the US National Institute of Diabetes and Digestive and Kidney Diseases and the National Library of Medicine. It provides comprehensive, evidence-based information on drug-induced liver injury (DILI), including clinical features, mechanisms of hepatotoxicity, case reports and references to primary literature (https://www.ncbi.nlm.nih.gov/books/NBK547852/). Omeprazole is metabolised mainly by CYP2C19, whereas ibuprofen is metabolised by CYP2C9 [72]. When melatonin saturates CYP1A2, its metabolism can be diverted to CYP2C19 and CYP2C9, leading to enzyme saturation and reduced clearance of omeprazole and/or ibuprofen, which could contribute to hepatotoxicity (Fig. 6). Although sertraline (LiverTox score of B) is mainly metabolized by CYP2B6 [69], it may have played a role in competing for CYP1A2, 2C9 and 2C19 [73], leading to the subsequent metabolic overflow of omeprazole and/or ibuprofen.
Fig. 6 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Hypothetical scheme of possible drug interactions that would have occurred in case 2. Melatonin competes with other substrates for binding sites to CYP2C19 and CYP2C9 enzymes, increasing the duration of liver exposure to these high liver toxicity drugs. The LiverTox index of each drug is indicated in brackets [64]. CYP, cytochrome P450
Case 3 was taking melatonin, tizanidine, nabiximol, acetaminophen, omeprazole and acetylsalicylic acid (ASA). Tizanidine, as melatonin, is almost exclusively metabolised by CYP1A2, making it a direct competitor for enzymatic processing. Although tizanidine (LiverTox score: C) rarely causes hepatotoxicity, its presence could have contributed to CYP1A2 saturation, along with nabiximol and acetaminophen, both minor substrates of CYP1A2. This could have redirected the melatonin metabolism to CYP2C19 and CYP2C9, leading to the accumulation of omeprazole and ASA, both classified as LiverTox scores: B and A, respectively (Fig. 7) [64]. Furthermore, as in case 1, excess NAPQI production from acetaminophen due to saturation of the glucuronidation and sulfation pathways may also have played a role in liver injury.
Fig. 7 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Hypothetical scheme of possible drug interactions that would have occurred in case 3. Melatonin promotes drug accumulation, some of which could be hepatotoxic, by competing as a substrate for the binding site of the different isoforms of CYP450 involved in liver catabolism in phase I reactions. On the other hand, the glucuronidation and sulfation pathways are also saturated by high melatonin levels, and the CYP systems metabolize more acetaminophen. This leads to increased NAPQI production and GSH depletion, increasing liver damage. The LiverTox index of each drug is indicated in brackets [64]. CYP, cytochrome P450; NAPQI, N-acetyl-p-benzoquinone imine; UGT, UDP-glucuronosyltransferase; SULT, sulfotransferase
On the contrary, the patient who was enrolled in the study for the longest period (Mel 4), did not exhibit any signs of hypertransaminasemia throughout the 14-month treatment period, as confirmed by three biochemical evaluations (Table 3).
Interestingly, this patient had a greater than 50% reduction in plasma levels of ALT and AST levels after 12 months of melatonin treatment, consistent with previous reports on its potential hepatoprotective effects [38, 39]. Remarkably, this patient was the only one whose medications did not share metabolic pathways with melatonin (Fig. 4). Furthermore, the drugs that he was taking had low LiverTox scores: tamsulosin (D), dalfampridine (E) and hydroferol (E), suggesting that melatonin alone is unlikely to induce hepatotoxicity unless other hepatotoxic drugs accumulate.
In line with this interpretation, previous studies evaluating high-dose melatonin in other clinical contexts have not reported hepatotoxicity, even when the compound was co-administered with various medications. In ALS, melatonin (30–300 mg/day) was administered together with riluzole, amitriptyline, baclofen and antioxidant vitamins C and E [28, 29]. Among these, only riluzole shares hepatic metabolic pathways with melatonin, mainly involving the CYP1A2 and UGT enzymes [
Comments (0)