
Remember me

Epidemiological data indicate that up to 60% of patients with major depressive disorder (MDD) are receiving selective serotonin reuptake inhibitors (SSRIs) [1]. Despite adequate pharmacological treatment, approximately one-third of individuals with MDD do not achieve symptomatic remission, with even fewer achieving functional remission. Discontinuation of stable SSRI therapy can induce debilitating withdrawal symptoms, worsening of depression, and suicidality. Growing evidence supports that some psychedelics, for example psilocin, can induce fast and sustained depressive symptom improvement [2]. Owing to concerns about possible pharmacodynamic interaction, such as QT-time prolongation, serotonergic toxicity, or attenuation of psychedelic effects [3], SSRIs have been discontinued before psychedelic administration in most published clinical trials, except in two healthy volunteer studies [4, 5] and one open-label study with psilocybin for depression [6]. This study aimed to generate preliminary data on the effects of intranasal 5-MeO-DMT, a short-duration psychedelic, in participants with treatment-resistant depression (TRD) on stable doses of an SSRI.
This 12-week open-label, single-center, ascending-dose trial evaluated the safety, tolerability, and effects of a single intranasal dose of 10 or 12 mg 5-MeO-DMT (5-methoxy-N,N-dimethyltryptamine) on symptoms of depression in participants aged 18–75 years diagnosed with moderate-to-severe MDD (either first or recurrent episode), defined as a baseline Montgomery–Asberg Depression Rating Scale (MADRS) score ≥ 24 and TRD defined as failure to respond to an adequate dose and duration of at least two antidepressants. The clinical trial registration information is as follows: NCT05660642: An Open-Label Study to Evaluate the Safety, Tolerability and Pharmacodynamics of BPL-003 in Patients with Treatment Resistant Depression, https://clinicaltrials.gov/study/NCT05660642).
Participants were on a stable, adequate dose of one of four SSRIs—citalopram, escitalopram, sertraline, or fluoxetine—and deemed otherwise healthy on the basis of medical history, physical examination, electrocardiogram (ECG), hematology, biochemistry, and coagulation laboratory tests. Key exclusion criteria included a history of any medical condition with risks associated with transient increases in blood pressure and heart rate; current or a history of schizophrenia, psychotic disorder including psychotic depression, bipolar disorder, delusional disorder, schizoaffective disorder, or any other severe psychiatric disorder assessed via the Mini International Neuropsychiatric Interview and McLean Screening Instrument for Borderline Personality Disorder.
After completing the screening period, eligible participants underwent three preparatory psychological support sessions over approximately 2 weeks before the treatment session. Intranasal 5-MeO-DMT was administered in accordance with established safety practices for psychedelic research [7]. Three post-dosing psychological support sessions were conducted during the 2 weeks following the treatment session. The psychological support provided by a trained therapist was standardized and nondirective, and included preparation before, support during, and integration after the dosing. Participants were followed up for 12 weeks after dosing.
Adverse events (AEs) were recorded throughout the trial. Suicide risk assessment was conducted via the Columbia-Suicide Severity Rating Scale (C-SSRS). Cardiac telemetry and vital signs were tracked during the dosing session. Readiness for discharge was assessed every 30 min starting at 90 min post dose. Symptom improvement was determined by changes in the MADRS.
A safety review committee evaluated the findings in the initial cohort receiving a dose of 10 mg BPL-003 (the propriety formulation of intranasal 5-MeO-DMT evaluated in this trial) to determine if it was appropriate to escalate the dose to 12 mg. Statistical analyses for this open-label exploratory study were primarily descriptive, and no a priori hypotheses were tested.
A total of 12 participants, 6 in each of the two dose cohorts, were treated with intranasal 5-MeO-DMT between 22 February 2024 and 02 January 2025. Participants were aged 31–55 years, seven were female (5–10 mg, 2–12 mg), five were male (1–10 mg, 4–12 mg), the majority were white (11/12), and one was mixed race (White and asian). Demographics are presented in Supplementary Table 1. The mean time to MDD diagnosis was over 15 years in both dose cohorts, and the mean duration of the current episode was 227.8 (176.1) months in the 10 mg group and 123.7 (117.1) months in the 12 mg group. All participants had been on SSRI treatment for at least 5 months before being dosed with 5-MeO-DMT.
A history of suicidal ideation was reported in 8/12 (67%) participants, two of whom had prior suicidal behaviors. No occurrences of suicidal ideation were reported during the trial.
Drug-related treatment-emergent AEs (TEAEs) included administration-site (intranasal) symptoms and gastrointestinal effects occurring and resolving on the dosing day (Table 1). One participant reported feeling disoriented, dizzy, and nauseous as well as experiencing a pseudo-hallucination described as if feeling out of their body the day after dosing while reflecting on the dosing experience and listening to music similar to that played in the treatment room; the symptoms resolved completely within 15 min and did not recur. No other post-acute symptoms were reported. No severe TEAEs or serious AEs (SAEs)—defined as an AE that is life-threatening or results in death, inpatient hospitalization, or prolongation of existing hospitalization; results in significant disability or incapacity; constitutes a congenital defect; or requires intervention to prevent one of these outcomes—were reported.
Table 1 Drug-related treatment-emergent adverse eventsTransient elevations in blood pressure, with no accompanying cardiovascular symptoms, occurred following dose administration. The mean blood pressure increased from a pre-dose level of 101.6/63.2 (systolic: standard deviation [SD] 12.5, range 89–126; diastolic: SD 8.20, range 49–73) mmHg to peak levels at 10 min post dose of 132/81.3 (systolic: SD 27.53, range 102–182; diastolic: SD 6.44, range 72–91) mmHg in the 10 mg cohort and from a pre-dose level of 106/65.9 (systolic: SD 8.83, range 95–116; diastolic: SD 6.49, range 55–74) mmHg to peak levels at 10 min post dose of 136/85.2 (systolic: SD 15.68, range 120–163; diastolic: SD 9.89, range 73–99) mmHg in the 12 mg cohort. Blood pressure returned to baseline levels after 90 min in both cohorts.
The mean time participants were assessed as ready for discharge post dose was 102 (range 94–130) min in the 10 mg cohort and 96 (range 94–104) min in the 12 mg cohort.
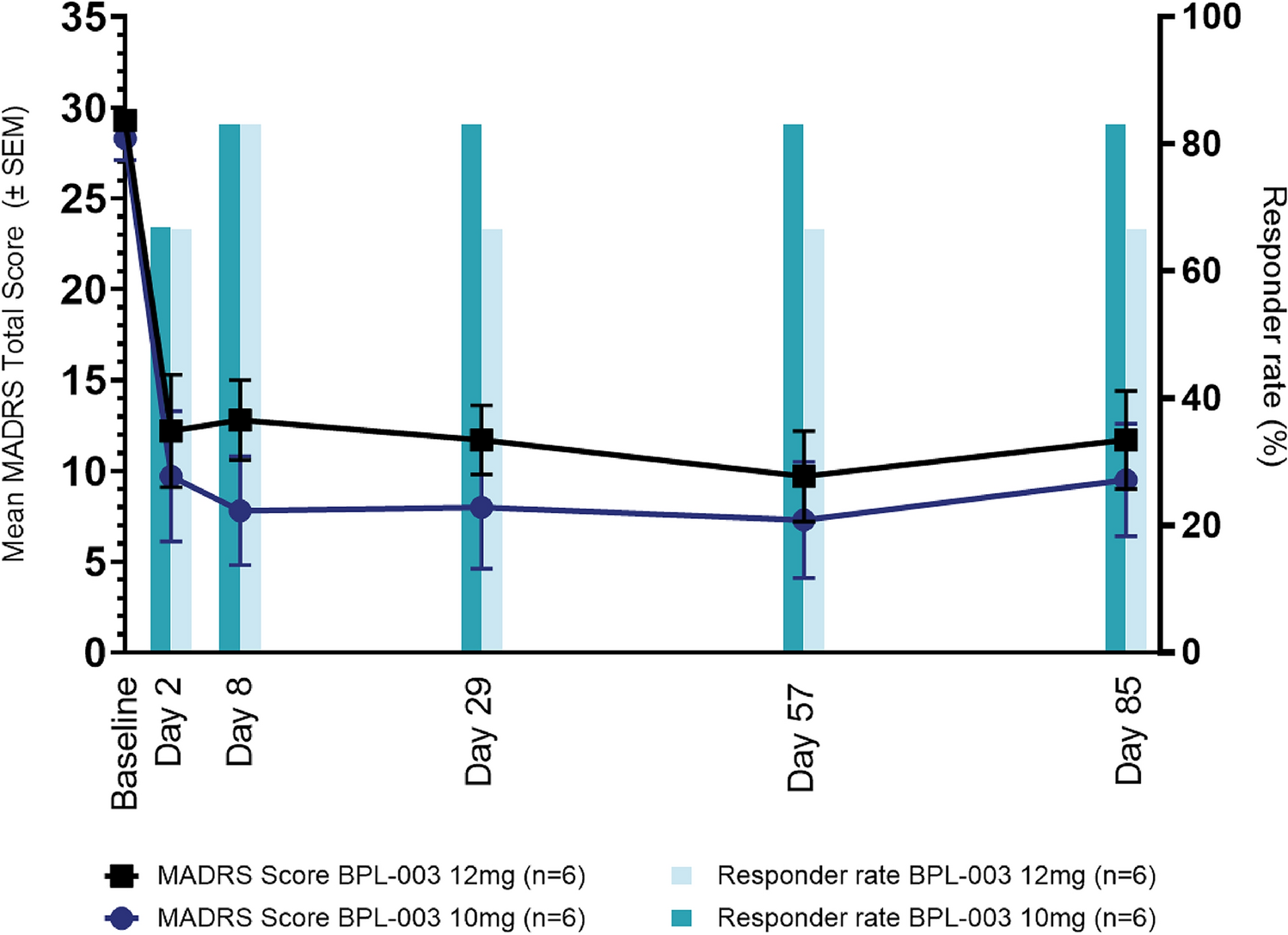
Rapid and sustained reductions in MADRS scores were observed (Fig. 1). Collectively, 66.7% (4/6) of participants were responders, defined as a ≥ 50% reduction in score, at the first post-dose assessment, on day 2 and 83% (5/6) were responders at day 85 in the 10 mg cohort. Similar results were found in the 12 mg cohort, with 66.7% (4/6) responders at days 2 and 85. Reductions in all MADRS items occurred at all post-dose assessments. The MADRS-6 subscale (including core depression symptoms of apparent sadness, reported sadness, inner tension, lassitude, inability to feel, and pessimistic thoughts) decreased from 19.2 (SD 1.5, range 7–21) at baseline to 7.3 (SD 7.1, range 1–19) at day 2 and 6.2 (SD 5.6, range 0–15) at day 85 in the 10 mg cohort and from 21 (SD 2.1, range 17–23) at baseline to 10 (SD 5.8, range 4–18) at day 2 and 9.3 (SD 5.4, range 0–16) at day 85 in the 12 mg cohort.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.MADRS Total Score and responder rate
The results of this first phase 2a clinical trial of intranasal 5-MeO-DMT administered adjunctively to SSRIs demonstrated acceptable safety and tolerability with promising improvements in depressive symptoms. The safety findings are in line with those reported in trials of intranasal 5-MeO-DMT administered to healthy volunteers [8] and as monotherapy to participants with TRD. The dose range evaluated does not indicate attenuation of efficacy when dosed adjunctively to SSRI.
A recent systematic review and meta-analysis of studies of classic psychedelic administration in monitored clinical or research settings reported that classic psychedelics were generally well tolerated [9]. In participants with preexisting neuropsychiatric disorders, 4% of experienced SAEs were worsening depression, suicidal behavior, psychosis, and convulsive episodes. No SAEs were reported in this trial; however, the small sample size limits the conclusions that can be drawn.
Psychedelics have demonstrated potential for providing rapid and long-lasting relief from symptoms in individuals with depression and are currently being explored as a treatment option. Short-duration psychedelics may offer more scalable and cost-effective clinical applications as compared with long-duration psychedelics [10]. The readiness for discharge assessed at around 2 h post dose is consistent with findings in other trials of intranasal 5-MeO-DMT.
This trial has clear limitations, including a small sample size and the absence of a control group. In addition, the study population was predominantly White with limited ethnic diversity. Limited diversity of participants is a common finding in clinical trials of classical psychedelics that needs to be resolved. The results of this trial may not be generalizable to concomitant use of intranasal 5-MeO-DMT with all SSRIs, particularly in consideration of the time since diagnosis and duration of the current episode in the trial participants.
In conclusion, the results of this first phase 2a study of intranasal 5-MeO-DMT administered concomitantly with SSRIs in participants with TRD demonstrated a single dose of 10 mg or 12 mg was well tolerated and indicate encouraging exploratory evidence for a sustained improvement in depression. Additional data are needed, supporting the case for controlled clinical trials in this population.
Comments (0)