
Remember me
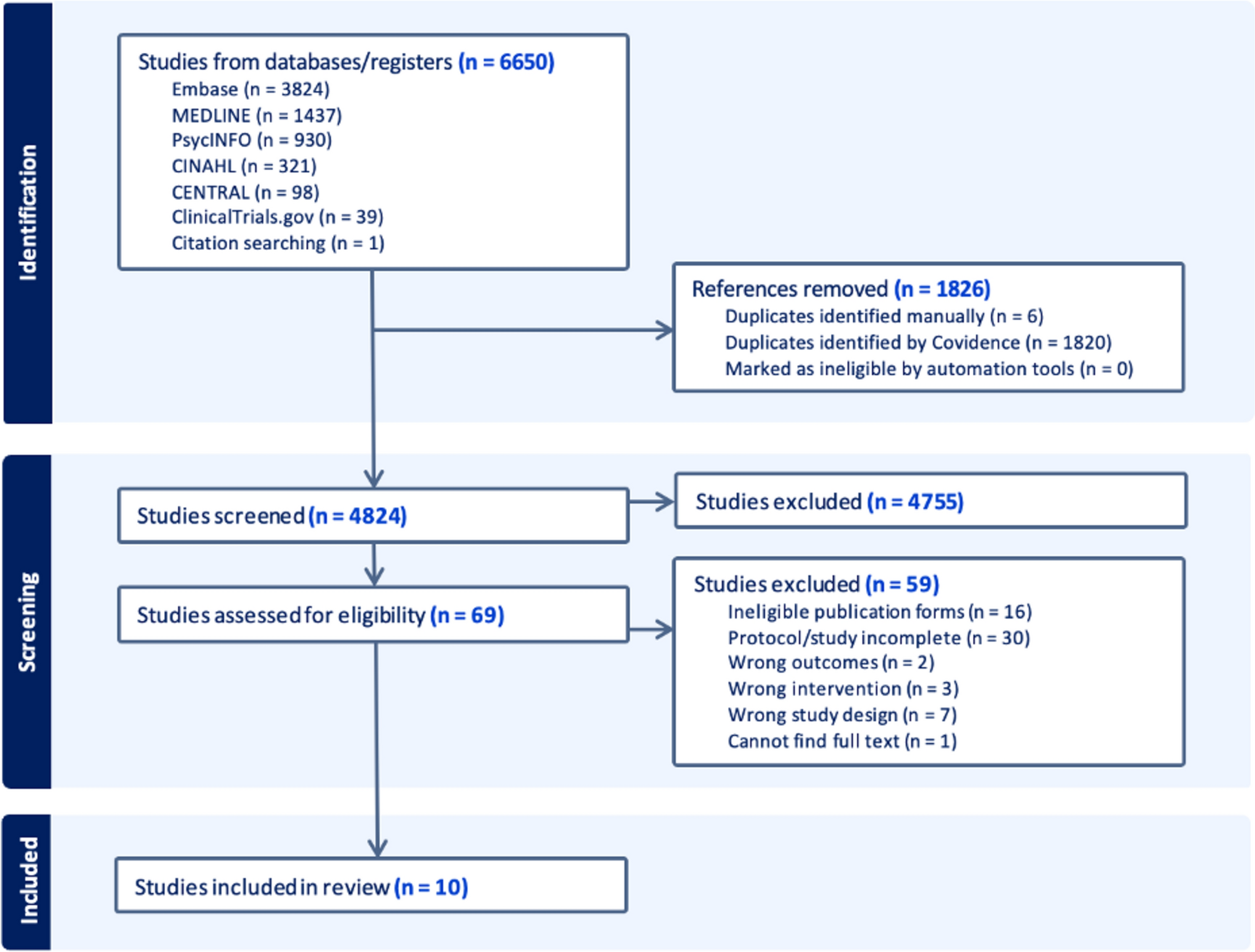

SEL and BRV were developed in parallel by UCB Pharma. Both drugs underwent early-phase clinical trials (phase I and phase IIa) with oral administration, but only BRV was subsequently evaluated in large phase III trials. Results of early-phase clinical trials with oral administration of SEL are reported in the following sections.
5.1 Tolerability of Seletracetam After Oral Administration in Healthy VolunteersThe tolerability of SEL following single and multiple doses was evaluated in healthy volunteers (Table 3). Overall, SEL was well tolerated following single oral doses from 2 mg to 600 mg and following multiple oral doses of 200 mg twice daily [43].
Table 3 Early-phase clinical trials with oral seletracetam. A total of 171 participants were treated (53 healthy volunteers and 118 patients with epilepsy)Subjects in the single-dose study reported adverse events typical of ASMs, including dizziness, somnolence, nausea, and headache [4]. The incidence of dizziness tended to increase at doses of ≥50 mg; however, nausea, somnolence, and headache did not seem to be dose-related. All the adverse events reported were of mild or moderate intensity, and the doses tested appeared to be well tolerated.
In the repeated-dose study, the subject-reported adverse events were similar to those observed in the single rising dose study, with CNS adverse events reported most frequently, the majority of which were of mild to moderate intensity. In general, these adverse effects occurred within 1 hour of initial dosing and decreased in incidence with subsequent dosing [4].
5.2 Pharmacokinetics and Metabolic Profile of Seletracetam Following Oral Administration in Healthy VolunteersThe pharmacokinetics of SEL were studied in healthy male subjects in a single rising dose study, with oral doses ranging from 2 to 600 mg [4]. SEL was rapidly absorbed, as demonstrated by a maximal plasma concentration (Cmax) that was reached within 1 hour after dosing in the majority of fasted subjects. Coadministration with a high-fat meal resulted in a delayed time to Cmax (median time delayed from 0.5 to 4 h after the dose) and a 39% reduction in Cmax but did not affect the overall extent of absorption. The disposition of SEL was characterized by linear pharmacokinetics over the 300-fold dose range studied. The volume of distribution was approximately 0.6 L/kg, which is close to that of total body water, indicating that SEL distributes to all tissues, including the brain. SEL plasma terminal half-life was approximately 8 h in young healthy male subjects; it did not vary with dose. The total apparent clearance was approximately 67 mL/min, or approximately 0.8 (mL/min)/kg; this is much lower than the hepatic blood flow (1500 mL/min), indicating a low extraction ratio by the liver.
A repeated-dose study was performed in 36 healthy male volunteers (Table 3). Subjects received either 20, 60, or 200 mg twice daily for 2 weeks. SEL was shown to have predictable pharmacokinetics. Dose proportionality was confirmed for elimination and half-life. The metabolite concentrations were approximately 10-fold lower than those of the parent compound. After repeated dosing, no unexpected accumulation of either parent compound or metabolite was observed, and no autoinduction of SEL clearance occurred, confirming time-independent pharmacokinetics [4].
A study was conducted to investigate the excretion balance and metabolism of orally administered [14C]SEL (100 mg) in six healthy male volunteers [4]. Absorption of SEL administered as an oral solution was rapid and nearly complete, with 92% of radioactive tracer recovered in urine. The urine metabolic profiling indicated that, besides the parent compound, one major metabolite was identified (ucb-101596-1, the acidic metabolite) and two additional minor metabolites. At 168 h, 3.21% of the dose was recovered in the feces, and 91.9% of the dose was recovered in urine, reflecting a high absorption of the drug. In the urine, the unchanged compound (25%) and the major metabolite measured (53%) represented 78% of the dose. In plasma, radioactivity was measurable until 72 h after the dose for all subjects. The major radioactive component was the parent drug, representing generally > 90% of the circulating radioactivity up to 24 h after administration. The remaining radioactivity (up to 10%) was associated with ucb-101596-1, the acidic metabolite.
5.3 Tolerability of Seletracetam After Oral Administration in Epilepsy Patients5.3.1 Photosensitive EpilepsyOf 27 participants with photosensitive epilepsy in whom single oral doses (0.5–20 mg) of SEL and of placebo were administered, 18 participants reported adverse effects after SEL and four after placebo [44]. The most frequently reported adverse effects after SEL were somnolence (32%), dizziness (21%), headache (14%), and feeling drunk (7%). In participants with somnolence, this adverse effect started within one hour in six participants (at SEL doses of 0.5–10 mg) and at 2, 3.5, and 4 h after intake of 1, 10, and 20 mg in other participants, respectively. The duration varied from 19 min to 3 h (SEL doses between 0.5 and 20 mg) in six, while three other participants reported a duration of 4.5 (4 mg), 7 (2 mg), and 19 (1 mg) hours. Dizziness was reported by four other participants with onset between 15 min and 2.5 h, with duration between 23 min (SEL 10 mg) and 5.5 h (SEL 10 mg). No evident association was observed between the incidence of adverse effects reported after SEL administration and the dose or plasma level. All but one of the adverse effects observed were mild to moderate. One subject had severe somnolence after SEL 4 mg lasting 3 h. All treatment-emergent adverse effects were resolved before the end of the study. No serious adverse effects occurred. No effects on mood were observed.
5.3.2 Focal EpilepsyTwo phase IIa open-label studies evaluated the safety, tolerability, and efficacy of SEL adjunctive therapy in adult participants with focal epilepsy (Table 3). The full results of the studies have not been published, but study protocols and results have been posted on the ClinicalTrials.gov site (identifiers NCT00152503 and NCT00152451).
Study NCT00152503 enrolled 59 adults (aged 18–65 years) from May 2005 to May 2006. It was an open-label, exploratory, dose-escalation phase II study of the safety, tolerability, and efficacy of SEL capsules. SEL was administered in doses of 10, 20, 40, and 80 mg twice daily (daily doses of 20–160 mg) as an add-on treatment to patients with drug-resistant focal epilepsy (previously called refractory partial epilepsy) with continued seizures while receiving one to three concomitant ASMs, including LEV. Following 4 weeks at baseline, subjects were treated with SEL for 11 weeks. They were up-titrated every 2 weeks from 20 to 160 mg/day until the maximum tolerated dose was reached. They were maintained at this dose until the end of the 8th week, followed by a 3-week down-titration period.
Of 59 subjects enrolled (52% women), 55 subjects completed the study, and four subjects stopped the study because of adverse events, although the data posted on the site do not identify which adverse effects led to discontinuation, nor whether or not they were treatment-emergent adverse events. SEL appeared well tolerated. There were three serious adverse events, seemingly unrelated to the medication (skin cancer, convulsion, and unstable angina). Side effects with > 5% incidence included dizziness (22%), nausea (20%), headache (15%), fatigue, and somnolence (14% each), followed by nasopharyngitis (12%), vomiting, and urinary tract infection (10% each), cough (8%), nystagmus, diarrhea, abdominal pain, and pharyngolaryngeal pain (7% each) and, at 5% each, decreased appetite, bronchitis, convulsion, dyspnea, herpes simplex infection, irritability, sinus congestion, and tremor.
Study NCT00152451 (UCB study NO1101) enrolled 31 participants (48%), also from May 2005 to May 2006. It was also an open-label, exploratory, multicenter, dose-escalation study of the efficacy, safety, and tolerability of SEL at doses of 10 mg, 20 mg, 40 mg, and 80 mg twice daily (total daily dose of 20–160 mg) with the same 4-week baseline, 8-week up-titration, and 3-week down-titration periods as study NCT00152503. Adult subjects (aged 18–65 years; 48.4% females) with drug-resistant focal epilepsy were treated with one, two, or three ASMs. Like the other study, participants were up-titrated every 2 weeks until the maximum tolerated dose was reached and were maintained at this dose until the end of the 8-week up-titration period, followed by a 3-week down-titration. Of the 31 participants who started the study, 27 completed it. Four stopped early because of adverse events, although the results posted on the ClinicalTrials.gov site do not disclose which adverse effects led to treatment discontinuation or whether they were treatment-emergent adverse events. The most common adverse effects present in > 5% of participants were dizziness (23%), headache and depressed mood (12.9% each), anxiety, decreased appetite and upper respiratory tract infection (10% each), and fatigue, gait ataxia, abnormal coordination, nystagmus, insomnia, irritability, nervousness, and nasal and sinus congestion, at 6% each.
5.4 Pharmacokinetics of Seletracetam Following Oral Administration in Epilepsy PatientsRepeated blood samples were taken in the phase IIa POC study in photosensitive patients, thus allowing for the determination of the pharmacokinetics of SEL in the presence and absence of comedication with ASMs [44]. After each dose (0.5–20 mg) of SEL, maximal plasma concentrations were reached within approximately 2 h and were followed by a mono-exponential decline. The concentration decreases after Cmax values were parallel for all doses as evidenced on the semi-logarithmic plot, implying a similar terminal half-life of ~ 8 h across doses. Furthermore, plasma concentrations appeared to increase in a linear proportion with the administered dose, as reported previously for healthy volunteers [4]. Figure 4A illustrates the linear regression between Cmax and oral dose in the photosensitive participants. Figure 4B shows the linear regression between the area under the plasma concentration curve (AUC; a measure of total drug exposure) and oral dose of SEL in these participants. The linear, time-independent pharmacokinetics of the drug, combined with a rapid and almost complete absorption, indicate that SEL has a straightforward pharmacokinetic profile.
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Pharmacokinetics of seletracetam (SEL) following administration of single oral doses in 27 patients with photosensitive epilepsy. Data are shown as means ± standard deviation (SD). A Maximal plasma concentration (Cmax) of SEL following doses of 0.5, 1, 2, 4, 10, and 20 mg. Note the linear relationship between dose and Cmax, resulting in a highly significant correlation between the two variables. B Area under the plasma concentration–time curve (AUC) determined following oral doses of 0.5, 1, 2, 4, 10, and 20 mg of SEL. Note the linear relationship between dose and AUC (i.e., total drug exposure), resulting in a highly significant correlation between the two variables. See Kasteleijn-Nolst Trenité et al. [44] for additional pharmacokinetic parameters of SEL
Interestingly, when comparing the median time to the first response on the photoparoxysmal electroencephalographic (EEG) response (PPR; see Sect. 5.5.1) with plasma levels of SEL, the first response was observed before reaching the time of maximal plasma levels (tmax) at 0.5–1 h for 1–20-mg doses. The duration of response for the same dose was much longer than the half-life, and ranged from 16 to 31 h. This suggests that very low plasma levels of SEL are sufficient to produce an effect quickly and to maintain it for a long time. Examples of two participants are illustrated in Fig. 5, demonstrating the rapid onset of the anti-PPR effect and the long duration of the effect.
Fig. 5 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Example of two individual photosensitive epilepsy patients who were treated with seletracetam (SEL). In each trial, the patient received a placebo (day − 1; left part of each graph) and SEL (day 1; right part of each graph). Placebo or SEL were orally administered immediately after predrug (PD). The patient shown in A did not receive comedication with antiseizure medication (ASM), while the patient in B received valproate (VPA) on a chronic basis. The effect of oral intake of SEL on the photosensitivity range (upper and lower photosensitivity limits in Hz, depicted as a bar) is shown. The limits themselves are graphically expressed as small circles. The left y axis shows the photosensitivity in Hz, while the right y-axis shows the plasma drug concentration of SEL (in ng/mL) or VPA (in µg/mL). Drug levels are indicated by the dashed (VPA) or solid (SEL) lines. SEL (2 or 20 mg) completely abolished the photoparoxysmal response in both patients. Note the rapid onset and long duration of the effect. The two patients are from the trial published by Kasteleijn-Nolst Trenité et al. [44]
Most of the participants were on steady-state treatment with one or two ASMs. Data on plasma levels of these ASMs did not suggest obvious pharmacokinetic interactions between these ASMs and SEL [44].
5.5 Efficacy Data After Oral Administration of SeletracetamThree clinical studies have been performed with orally administered SEL, including a phase IIa POC trial in participants with photosensitive epilepsy and two phase IIa add-on studies in patients with focal epilepsy (Table 3).
5.5.1 POC Phase IIa Trial in Patients With Photosensitive EpilepsyThe photosensitivity model has become a widely accepted POC model for testing of diverse new ASMs [45]. Its utility rests on a read-out that is directly related to epilepsy, namely, reflex-induced epileptiform discharges in the EEG of patients with reflex epilepsy in whom there is a tight relationship between reflex photosensitive epilepsy and PPR to intermittent photic stimulation (IPS). PPR is suppressed by ASMs of diverse mechanisms of action and of diverse indication targets, including focal epilepsy, acute rescue therapy, or REST [45]. Data obtained in trials in photosensitive patients are useful to inform dose finding and effective plasma levels of an investigational drug for subsequent clinical trials in other patient populations or with other routes of administration (see Sect. 6).
The primary objective of the POC phase IIa trial with SEL was to identify the lowest single oral dose of SEL producing suppression of the IPS-evoked PPR in photosensitive epileptic subjects [44]. A secondary objective was to assess the relationship between plasma concentrations of SEL, changes in the photosensitivity frequency range, time of onset, and duration of the effect (see also Sect. 5.4). In this multicenter, single-blind, phase IIa study, adults with photosensitive epilepsy, with and without concomitant ASM therapy, underwent IPS under three eye conditions (at eye closure, eyes closed and eyes open) after a single oral dose of placebo (day − 1) or SEL (day 1; 0.5, 1, 2, 4, 10, or 20 mg). Complete suppression was a standardized photosensitivity range (SPR) reduction to 0 over one or more time points for all eye conditions. Partial suppression was a ≥ 3-point reduction over three or more testing times versus the same time points on day − 1 in one or more eye condition. In addition, pharmacokinetics and safety were assessed. Of 27 evaluable participants, nine reentered to receive a second drug exposure 1–6 months later, providing a total of 36 individual exposures. At all doses administered, even the lowest, several subjects reached a complete abolishment of PPR, with a rapid onset of effect. Overall, complete abolishment of PPR was obtained in 40–71% of the participants; the effect increasing with the dose. Comparing effective doses to suppress PPR, SEL was at least 1500 times more potent than LEV and 10–20 times more potent than BRV. The effects of SEL in two individual participants are illustrated in Fig. 5, demonstrating the rapid onset and long duration of SEL’s effect on PPR.
Concerning the relationship between plasma concentrations of SEL and its effect on PPR, a PPR-suppressing effect was already observed in some participants at the lowest dose (0.5 mg), at which Cmax was only ~ 13 ng/mL (Fig. 4A), underlining the high potency of the compound.
This POC study in photosensitive epilepsy patients showed that SEL is a promising ASM candidate, one with high potency, straightforward pharmacokinetics, and good tolerability in epilepsy patients. Photosensitive POC trials are useful for quantitatively predicting efficacy in focal or generalized epilepsies [45]. It is worth noting that SEL is the only non-BDZ ever tested in the human photosensitivity model that exerts effects on PPR at doses as low as effective BDZ doses.
5.5.2 Comedication With Levetiracetam Does Not Counteract the Effect of Seletracetam in Patients With Photosensitive EpilepsyMost (78%) of the participants in the study of Kasteleijn-Nolst Trenité et al. [44] were on comedication with one or two ASMs (including LEV, lamotrigine, valproate, topiramate, carbamazepine, phenobarbital, and phenytoin) that did not suppress the PPR response in these participants (see Fig. 5B). However, a group of six participants was not taking any ASM, and groups of similar size received different ASM comedications, thus allowing the determination of which, if any, of the ASMs reduced (or increased) the effect of SEL on PPR in individual participants [46]. Overall, a response to SEL was seen in 32 of the 36 exposures (Fig. 6; right column). In participants without any comedication, SEL completely suppressed PPR in 86% of the exposures (see Fig. 5A as an example). In participants on comedication with LEV, complete suppression was only observed in 33% of the exposures, which, however, was not statistically significantly different from participants without comedication (Fig. 6). Overall, in 78% of the SEL exposures in participants on concomitant LEV, a response (either partial or complete) was observed, indicating that comedication with LEV may reduce, but not abrogate the effect of SEL. As discussed in Sect. 2.1, the unique combination of effects on both SV2A and HVACCs may explain why SEL inhibits PPR even in the presence of LEV. This finding may suggest that in clinical practice, the two drugs could be combined and yet derive benefits from SEL. Similarly, none of the other ASMs examined in the phase IIa POC trial significantly counteracted the effect of SEL (Fig. 6). Indeed, given the fact that the PPR in these participants was resistant to treatment with steady-state doses of ASMs (see Fig. 5B as an example), the study shows that ASM failure could be overcome with add-on treatment with SEL in most (32/36) participants.
Fig. 6 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Effects of comedication with antiseizure medications (ASMs) on the efficacy of seletracetam (SEL) to suppress the photoparoxysmal EEG response (PPR; eye closure) after intermittent photic stimulation in patients with photosensitive epilepsy. PPRs were analyzed by an independent central EEG reader. Overall, SEL was tested in 36 exposures in 27 patients. SEL was tested following oral administration of single doses, ranging from 0.5 to 20 mg. Since the same dose range was tested in all subgroups, all values are shown together for each group. Data are illustrated as complete suppression of PPR, partial suppression of PPR, or no suppression of PPR for the following groups: SEL without ASM comedication; SEL in patients comedicated with levetiracetam (LEV); SEL in patients comedicated with lamotrigine (LTG); SEL in patients comedicated with valproate (VPA); SEL in patients comedicated with other ASMs (carbamazepine, topiramate, phenobarbital, phenytoin); and all SEL exposures. The effect of SEL seemed to be highest in the group without ASM comedication; however, statistical analysis of the data by Barnard’s test did not indicate any significant intergroup differences. Data are from Löscher et al. [46]
5.5.3 Phase IIa Add-on Trials in Patients With Drug-Resistant Focal Onset SeizuresTwo Phase IIa add-on trials with SEL were performed in participants with drug-resistant focal onset seizures (Table 3), but results of only one of these trials are available in the public domain.
In study NCT00152503 (n = 59), efficacy was evaluated as focal (partial) seizures during 7-day periods, comparing treatment periods during the up- and down-titration stages of the 11-week total treatment period with the 4-week baseline period. The evaluation included partial simple (focal preserved consciousness using current International League Against Epilepsy [ILAE] terminology [47]) seizures with a motor component, partial complex (focal impaired consciousness) seizures, and partial seizures with secondary generalization (focal to bilateral tonic-clonic seizures). SEL, administered as capsules in a twice-daily schedule, resulted in median percent seizure frequency reduction of 26% (20 mg/day), 32% (40 mg/day), 42% (80 mg/day), and 32% (160 mg/day) during the up-titration period. Of note, in this study, participants were on concomitant treatment with LEV, without seizure control, before entering the study. In the NCT00152451 study (n = 31), SEL treatment reduced seizure frequency (median percent reduction) by 40% (20 mg/day), 37% (40 mg/day), 28% (80 mg/day), and 40% (160 mg/day). During the up-titration period, 3% of participants achieved > 75 to < 100% seizure frequency reduction, and 6.5% achieved seizure freedom during treatment week 8, the last week of the up-titration period.
Comments (0)