Purpose
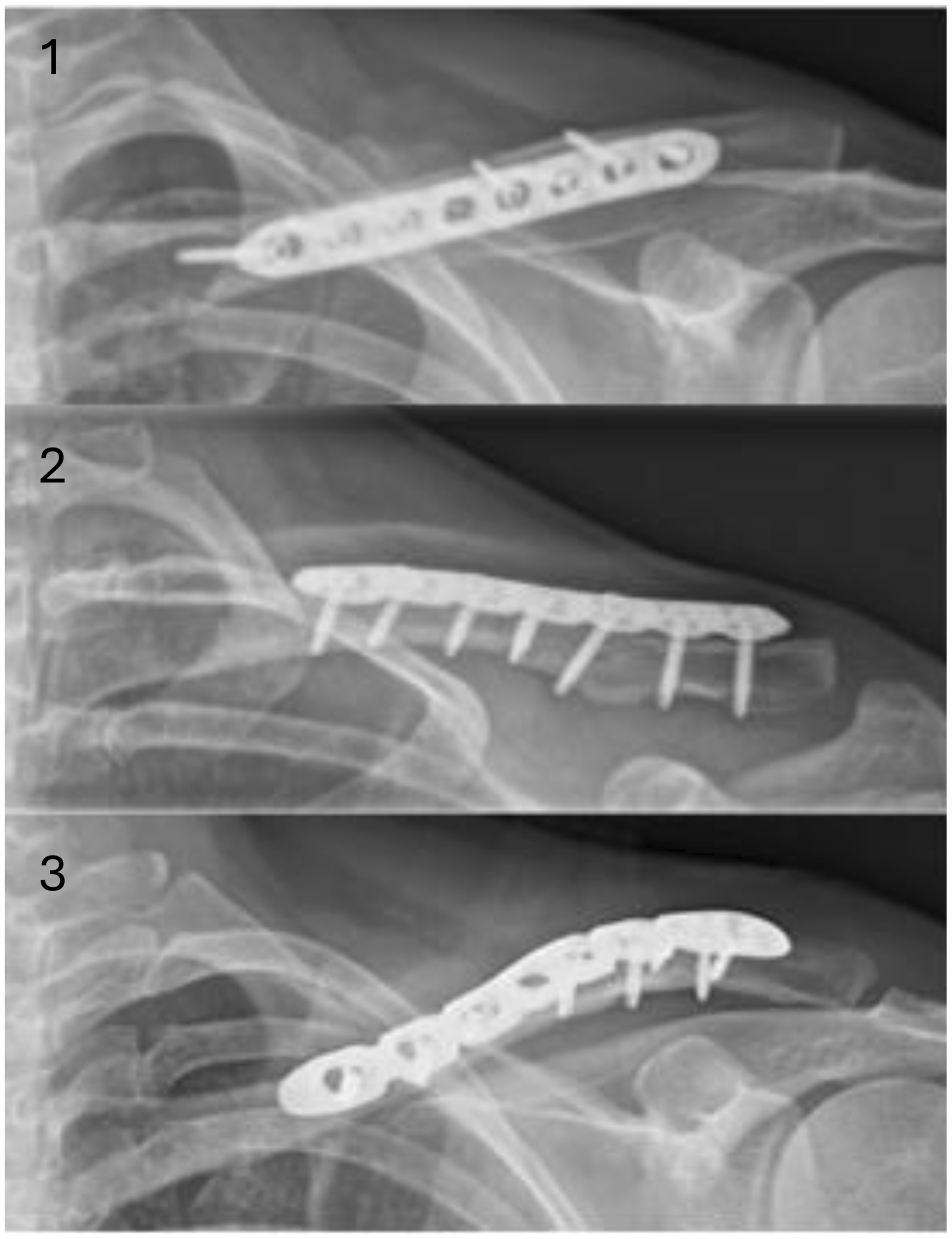
Plate osteosynthesis is a common procedure for clavicle shaft fractures. The plate can be placed in an anterior, anterior-superior, or superior position. This study aims to evaluate surgical treatment options regarding different plate positions for clavicle shaft fractures and to compare them regarding patient and perioperative characteristics, frequency of use, appearance of callus, complication rates and implant removal.
Methods
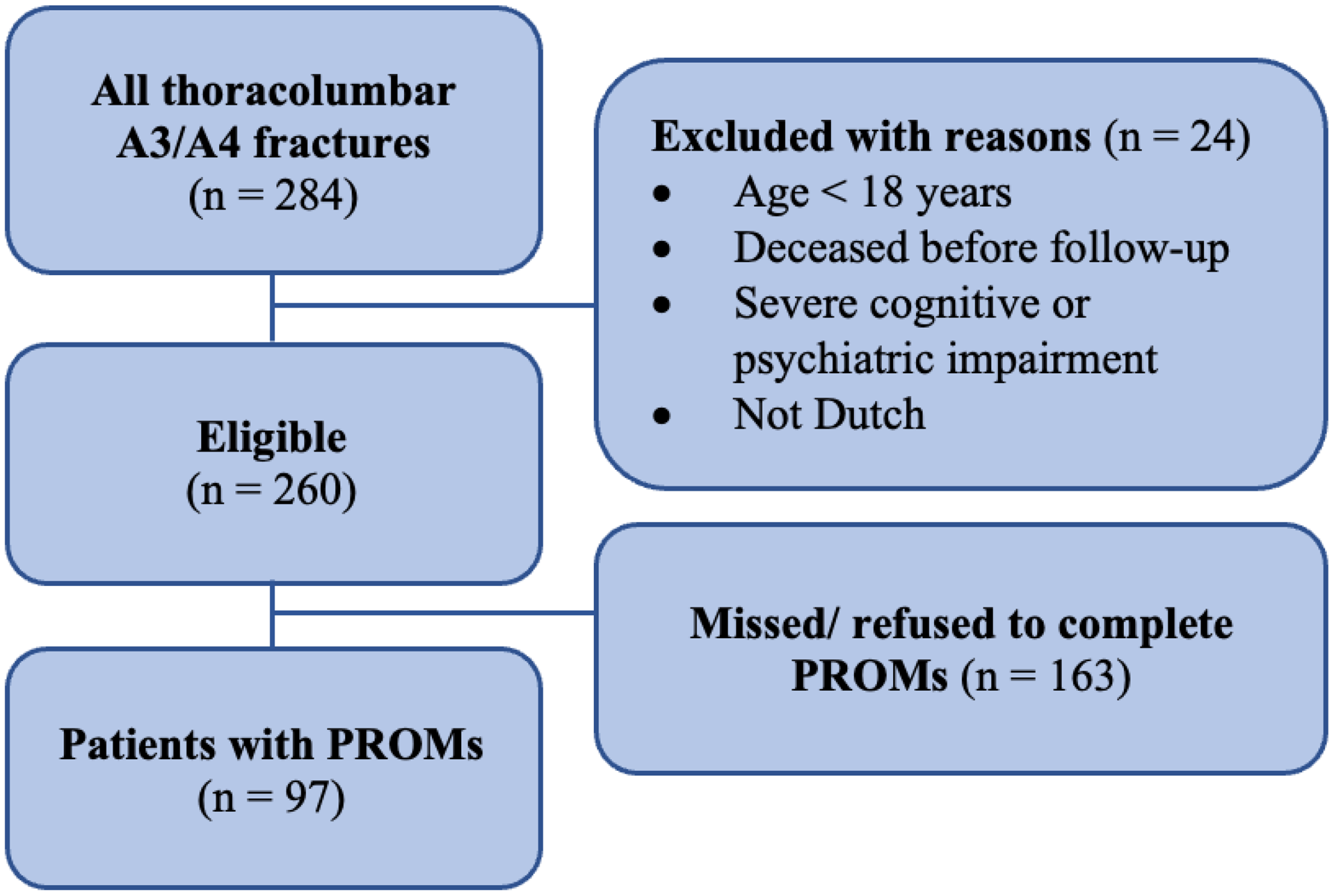
A retrospective cohort study of patients treated with plate osteosynthesis after clavicle shaft fracture between January 2016 and December 2024 at a Swiss level 1 trauma center was performed. Patients aged ≥ 16 years treated with anterior, anterior-superior or superior plate placement and availability of clinical follow-up data with X-ray were included. Presence of callus was subdivided into early (≤ 6 weeks), intermediate (> 6 to ≤ 26 weeks), and late (> 26 weeks).
Results
A total of 355 cases with a median of 41 years (range 17 to 90 years) (81.7%, n = 290 males and 18.3%, n = 65 females) were analyzed. The most commonly used plate position was anterior (92.4%, n = 328), followed by superior (5.6%, n = 20) and anterior-superior (2%, n = 7). Plate placement had no significant influence on operation time, callus formation, implant removal, or refracture after implant removal. Complications occurred in 6.2% (n = 22) of cases with a trend towards an increased complication rate with anterior-superior plate position (28.6%, n = 2), but the incidence of complications did not differ when comparing only anterior (5.5%, n = 18) and superior plate placement (10%, n = 2).
Conclusion
All three plate positions are valid surgical treatments for clavicle shaft fractures as similar results were observed with anterior, anterior-superior and superior plate placement. Further studies, particularly on anterior-superior plate fixation as well as patient reported outcome measures and clinical follow-up, are necessary to achieve optimal long-term surgical results.
Level of evidence
Level III, retrospective comparative study.



Comments (0)