This study demonstrates that treatment of children with distal forearm fractures in the Schede position is uncomplicated, effective, and safe. Given the high incidence of these fractures in children, treatment efficiency is of great importance. Many of these injuries can be managed conservatively with cast immobilization, with or without prior closed reduction, taking advantage of the excellent growth potential of the distal forearm.
The optimal joint position during immobilization remains a subject of debate, with various techniques described in the literature to prevent secondary fracture displacement and to achieve an anatomically correct and functional joint position at the end of treatment [5, 6]. In this study, the Schede cast immobilization technique was analyzed, as ligamentotaxis is intended to minimize mechanical stress on the fracture and reduce the risk of redislocation. Despite the recognized benefits of exploiting pediatric remodeling potential, concerns about retention therapy in the Schede cast have persisted for nearly a century. These concerns are based largely on adult data and contrast with positive clinical experience in pediatric practice.
The first reported case of iatrogenic carpal tunnel syndrome (CTS) following Schede cast immobilization of a distal radius fracture in adults was described by Abbott and Saunders [7], with subsequent studies attributing this complication to increased carpal tunnel pressure with wrist flexion [8, 9]. Although CTS is generally considered rare in children, it has been reported predominantly in association with distal radius pathology, particularly following trauma [19]. however, non-traumatic cases have also been described. In the present series, all cases of neurological irregularities were fully reversible, even in the presence of transient median nerve sensory disturbances. No impairment of two-point discrimination was observed, and there was no indication for surgical decompression. This favorable course may be explained by the higher tolerance of children and adolescents to elevated compartment pressures [10], which may allow more effective compensation for cast-induced increases in carpal tunnel pressure [8].
Temporary tingling paresthesia was observed in 2.4% of our patients and resolved spontaneously within days or after simple measures such as analgesia, cooling, or cast adjustment. The symptoms were generally non-dermatomal, likely reflecting tight casting or post-traumatic swelling. Notably, these paresthesias occurred more frequently in older children and in boys, possibly due to less flexible fascial sheaths in male adolescents [20].
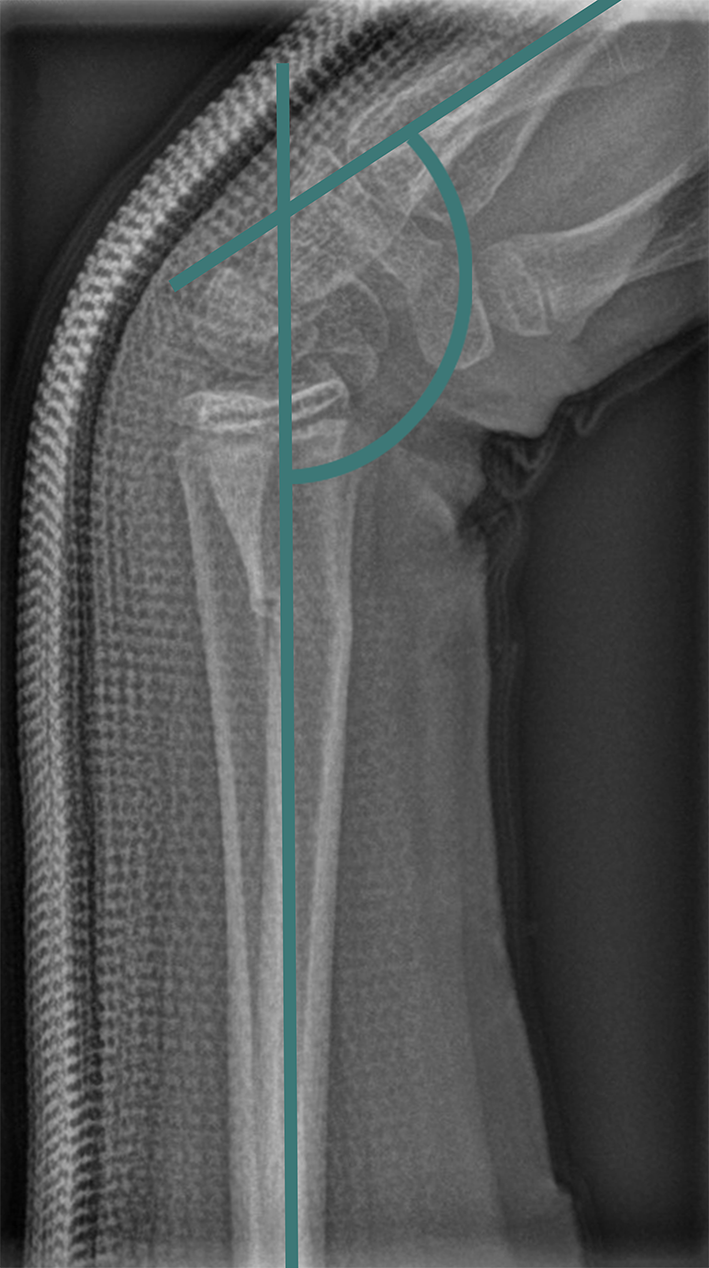
Prolonged movement restrictions were rare and resolved completely with physiotherapy. As expected, these limitations were more common in older children and in upper arm casts, likely reflecting decreased activity and slower recovery during puberty [13, 14]. Compared to adult studies reporting secondary dislocation rates of up to 39% [21], the rate of procedural change in our cohort was remarkably low at 2.9%, despite a higher proportion of radiographically detected secondary dislocations (12.4%). This discrepancy can be explained by two main factors. First, secondary dislocation was defined as a deterioration of ≥ 6.5° on follow-up radiographs, a deliberately low threshold chosen to enable early detection of subtle loss of reduction and to ensure comparability across participating centers with heterogeneous treatment protocols. Second, the distal forearm in children exhibits a high remodeling potential, allowing for considerable tolerance of mild secondary displacement without the need for surgical intervention. Patients with secondary dislocation were younger and more frequently treated with forearm casts, which were associated with lower mean flexion angles compared with upper arm casts. These findings support previous reports emphasizing the importance of adequate wrist flexion, with at least 45° recommended for Salter–Harris I and II fractures [22]. Our data suggest that this principle is also applicable to unstable meta- and diametaphyseal fractures, provided a flexion angle of at least 50° is maintained. CI values were generally high in our cohort (0.86 and 0.9), and measurement was challenging in certain cast types: dorsal casts do not allow valid CI determination, and in Schede casts, intentional joint flexion produces a cast curvature at the fracture level that can bias measurements. Previous studies have suggested that CI values above 0.8 are associated with secondary dislocation. In our study, however, nearly all measured CI exceeded this threshold, limiting variability and preventing meaningful analysis. Accordingly, no association between CI and secondary dislocation was observed, suggesting that CI may have a limited predictive role in this context [3, 23]. Concomitant ulnar fractures were not a statistically significant risk factor, although insufficient reduction remained a major predictor of secondary displacement [24]. In our cohort, conversion to closed reduction and Kirschner wire fixation was required in only 27 cases. This rate is substantially lower than those reported in previous studies, in which secondary procedural changes after an initial conservative treatment approach were described in up to 45% of cases [25, 26]. Limitations of this study include its retrospective and observational design without a standardized protocol. Due to the lack of a validated method for measuring ulnar abduction, only flexion was measured, although the Schede position includes both flexion and ulnar deviation. Nevertheless, the large sample size reflects real-world pediatric practice and demonstrates that Schede cast retention is a low-complication, conservative treatment for distal forearm fractures in children and adolescents, often avoiding surgical intervention. Compared with Kirschner wire fixation, Schede cast treatment is cost-effective, outpatient-friendly, and minimally invasive. Prospective studies, including randomized controlled trials, are needed to further validate these findings.



Comments (0)