Blood pressure variability in the ATACH2 study: evaluating a target range
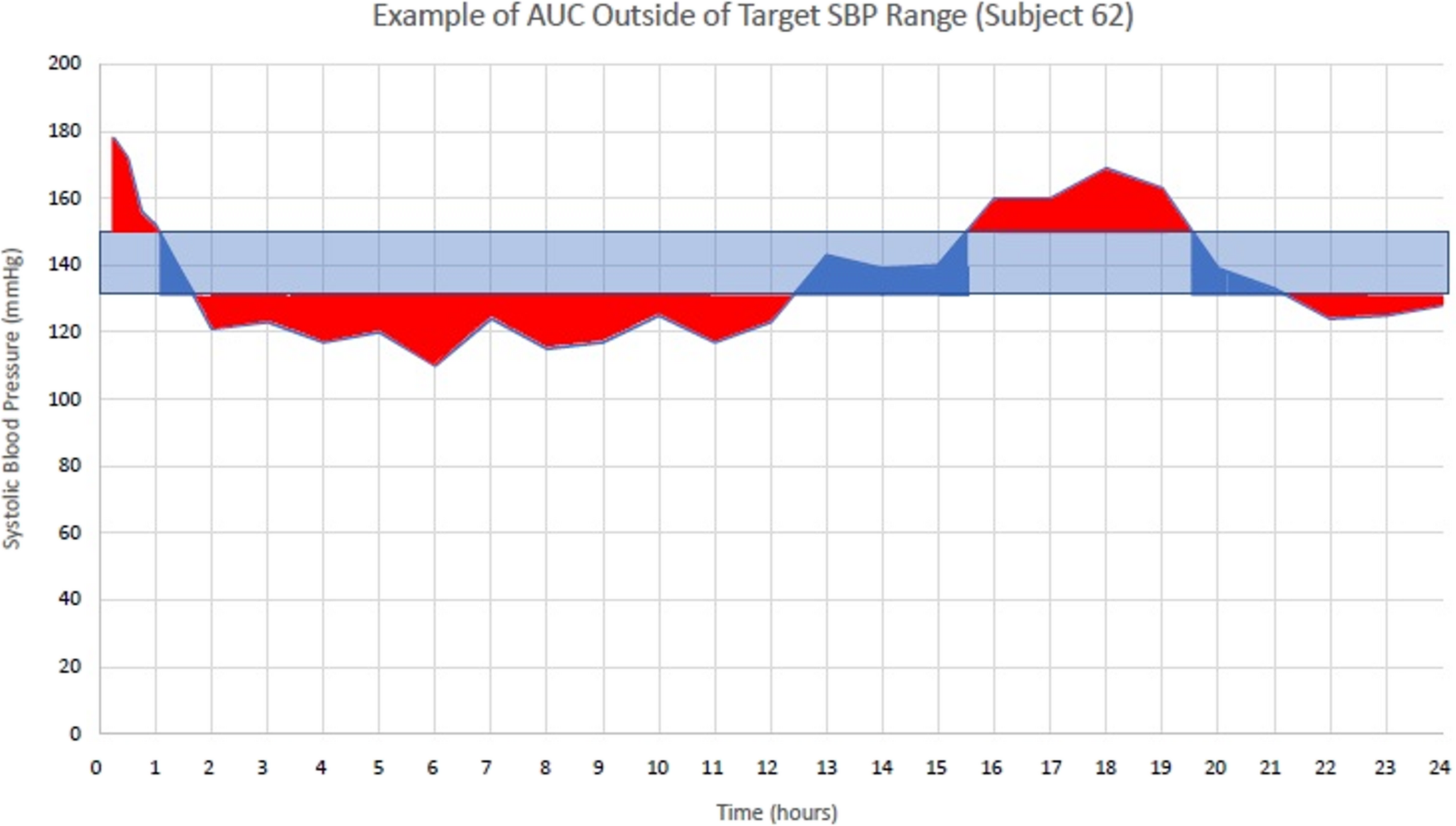
Blood pressure management after intracerebral hemorrhage (ICH) is a key part of early care to reduce complications and improve outcomes. Blood pressure variability (BPV) affects outcomes independently of achieving a specific goal. This study evaluated a novel method for describing variability—area under the curve (AUC)—and applied the guideline-suggested range for systolic blood pressure (SBP) to a prospective cohort previously studied. This was a post-hoc analysis of ATACH2 trial data. Variation outside the SBP range (130–150 mmHg) during the first 24 h was measured via AUC and compared to endpoints such as mortality, modified Rankin Score, and renal adverse effects. Multivariate regression analysis evaluated factors related to early neurologic outcome. 38.2% of SBP measurements were within the target range. Mean time to SBP nadir was 61 (SD 26.3) minutes, with a mean nadir SBP of 108.5 mmHg (SD 15.4). Median AUC in the standard cohort was 289 (IQR 188–400); in the intensive cohort, 291 (IQR 206–395, p = 0.478). Most of the AUC was below target in the intensive group and above in the standard group. Admission GCS, baseline NIHSS, and hematoma volume were significantly associated with poor 30-day outcomes; AUC outside the target SBP range was not (p = 0.569). SBP standard deviation (SD) and AUC showed modest correlation. AUC did not differ between cohorts and was not associated with neurologic outcome. Admission GCS, NIHSS, and hematoma volume were predictors of poor outcome after ICH.

Comments (0)