
Remember me

Lipomas are benign, adipose tissue–containing neoplasms that account for approximately half of all soft-tissue tumors, making them the most common subcutaneous neoplasm [14]. They most often present in adults during the fifth to sixth decades of life, although they may occur at any age. On MRI, lipomas are typically well-circumscribed, homogeneously fatty masses; they may display thin septations (< 2 mm) that may enhance after contrast administration [15]. Based on their location relative to the investing fascia of the deep muscles, lipomas are classified as either superficial or deep [14]. Most are encapsulated by a delicate fibrous capsule, but unencapsulated variants also exist. Additionally, regions of nonadipose tissue—such as fibrous stroma, cartilage, calcifications, or myxoid change can introduce internal heterogeneity, sometimes mimicking other soft-tissue neoplasms and complicating the differential diagnosis. Awareness of these imaging characteristics is crucial for accurate lesion characterization, appropriate differential diagnosis, and optimal therapeutic planning [14].
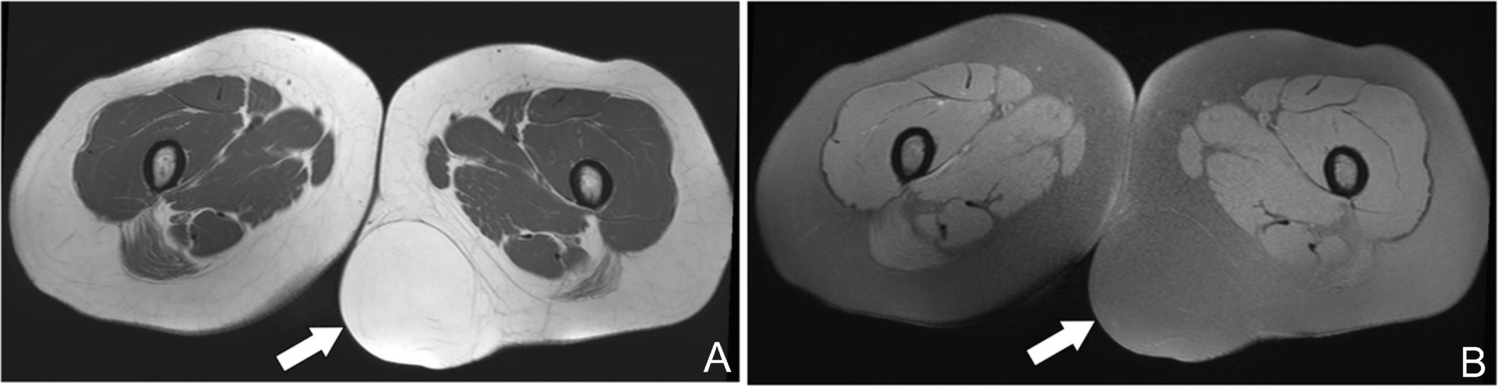
Superficial lipomaSuperficial lipomas arise within the subcutaneous fat, immediately above the superficial fascia, and typically mirror the signal intensity or attenuation of adjacent adipose tissue, which can make their margins difficult to appreciate on imaging. They may occur as well‐circumscribed, encapsulated masses or as nonencapsulated, infiltrative collections of fat, often referred to as lipomatosis, when a discrete capsule is absent (Fig. 1) [16]. According to current European Society for Medical Oncology (ESMO) guidelines, any homogeneous, superficial adipocytic lesion with a maximal dimension greater than 10 cm should be referred to a dedicated sarcoma center for multidisciplinary evaluation and consideration of image‐guided biopsy [17, 18].
Fig. 1
Axial MR images in a 49-year-old woman demonstrate an encapsulated superficial lipoma. (A) T1-weighted image and (B) fat-suppressed T2-weighted image show a well-circumscribed, homogeneously hyperintense mass within the subcutaneous fat (arrows), identical to subcutaneous fat signal in all sequences. A fine, low-signal-intensity fibrous capsule surrounds the lesion, confirming its encapsulated nature
Intra/intermuscular lipomaIntramuscular and intermuscular lipomas occur deep to the investing fascia, within or between muscle bundles. On imaging, they typically appear as well-defined, homogeneously fatty masses without thick septations (> 2 mm), nodular soft-tissue components, or non-adipose areas—features that, when present, raise concern for more aggressive pathology (Fig. 2). Whenever a deep adipocytic lesion deviates from these benign criteria, by exceeding 5 cm in maximal diameter, demonstrating internal heterogeneity, or showing suspicious septa or nodularity, lipoma variants, involutional changes, or, critically, liposarcoma must be considered (Fig. 3). In such cases, and per ESMO recommendations, referral to a dedicated sarcoma center for multidisciplinary assessment and image-guided biopsy is advised for any deep-seated adipocytic mass of the trunk or extremities [17, 18].
Fig. 2
Intramuscular lipoma in a 64-year-old man. (A) Radiograph of the right arm demonstrates a well-defined radiolucent soft-tissue mass (arrows). (B) Axial T1-weighted and (C) fat-suppressed T2-weighted MR images show a homogeneous intramuscular lesion isointense to subcutaneous fat, without evidence of internal non-fatty components (D,E) Sagittal post-contrast T1-weighted images confirm the absence of significant enhancement. (F) Gross pathological specimen reveals a yellow, lobulated mass with thin fibrous septa. (G) Photomicrograph (H&E, × 200) shows uniform mature adipocytes without atypia, consistent with benign lipoma
Fig. 3
Involutional changes in a longstanding thigh lipoma of a 21-year-old man. (A) Axial T1-weighted MR image demonstrates a large intramuscular lesion with signal intensity identical to subcutaneous fat, but containing thick, low-signal septations (arrows) that mimic features of an atypical lipomatous tumor. (B) Gross specimen of the resected mass reveals yellow, lobulated adipose tissue (*) traversed by prominent fibrous septa (S). (C) Photomicrograph (H&E, × 100) shows uniform mature adipocytes (*) separated by thick collagenous septa (S) without cytologic atypia, confirming benign involutional changes
Lipoma variantsLipoma variants encompass a heterogeneous group of benign adipocytic neoplasms whose imaging appearances often diverge from those of ordinary lipomas and may closely mimic well‐differentiated liposarcomas. According to the WHO classification, lipomas with a component of normal-appearing bone, cartilage, or fibrous connective tissue may be designated as osteolipomas, chondrolipomas, or fibrolipomas, respectively. However, these lesions are still considered as lipoma subtypes, included within the same nosological category as the purely adipocytic conventional lipoma. In contrast, there are several benign adipocytic neoplasms that are considered independent entities, including lipoblastoma, hibernoma, chondroid lipoma, angiolipoma, spindle cell/pleomorphic lipoma, atypical spindle cell/pleomorphic lipomatous tumor, and myolipoma [19]. Each entity exhibits unique histologic and clinical features, such as multilobulated architecture in lipoblastoma, brown fat attenuation in hibernoma, or prominent vascularity in angiolipoma, that can translate into atypical signal characteristics, septal thickening, or nodularity on MRI. Given this overlap with malignant adipocytic tumors, biopsy or complete excision is often warranted to establish a definitive diagnosis and guide management. Recognizing these variants in the differential diagnosis of any fat‐containing soft‐tissue mass is essential to direct appropriate multidisciplinary evaluation and treatment.
Lipoblastoma and diffuse lipoblastomaLipoblastomas are rare, benign adipocytic tumors that arise almost exclusively in infants and young children, with a male predominance of approximately 2–3:1. They most often involve the extremities and present in two forms: a well-circumscribed variant (lipoblastoma; Fig. 4) or an infiltrative, multicentric pattern known as diffuse lipoblastoma (Fig. 5) [20,21,22]. Histologically, these lesions contain immature, embryonal adipocytes that may, over time, differentiate into mature fat, occasionally resulting in spontaneous maturation to a conventional lipoma. Maturation occurs predominantly in the center of the tumor lobules, while immature tissue persists at the edges, consisting of lipoblasts in various stages of maturation, often within a myxoid matrix. These immature portions can be very similar histologically to myxoid liposarcoma, but in this tumor, the maturation pattern is reversed, that is, the more mature adipose cells predominate at the periphery of the lobules [19, 23]. On CT and MRI, lipoblastomas typically appear as predominantly fatty masses; however, their immature myxoid or cellular regions can produce nonspecific signal characteristics that overlap with those of liposarcomas, a malignancy exceedingly uncommon in the pediatric population [24]. Because imaging alone cannot reliably distinguish lipoblastoma from well-differentiated liposarcoma, correlation with patient age and prompt histopathologic confirmation are essential. The treatment of choice is complete local excision, aiming for clear margins while preserving surrounding structures to optimize functional outcomes and minimize recurrence [25].
Fig. 4
Lipoblastoma of the right inguinal region in a 1-year-old boy. (A) Clinical photograph demonstrates a palpable, well-circumscribed inguinal mass. (B) Coronal T1-weighted MR image and (C) fat-suppressed T2-weighted MR image show a predominantly fatty lesion with thick, irregular septa (arrows). (D) Axial CT image confirms a low-attenuation fatty mass with internal septations. (E) Axial T1-weighted and (F) post-contrast T1-weighted MR images further delineate the extent of the lesion and enhancement of the fibrous septa (arrows)(G) Gross specimen photograph reveals lobulated adipose tumor nodules separated by firm fibrous septa
Fig. 5
Infiltrative cervical lipomatous lesion. (A) Contrast-enhanced CT shows a fat-attenuation mass in the left neck containing streaky higher-density areas and extending through the neural foramina, causing bony enlargement and rightward displacement of the dural sac (arrows). Axial T1-weighted image (B) and axial (D) and coronal (E) T2-weighted MR images confirm a predominantly fatty lesion with interspersed thick septa (C) Axial post-contrast T1-weighted MR images demonstrate heterogeneous enhancement of the thick fibrous septations. (F) Photomicrograph (H&E, × 200) reveals mature adipocytes arranged in lobules separated by fibrous septa, with scattered spindle cells, lipoblasts, and a myxoid stromal background
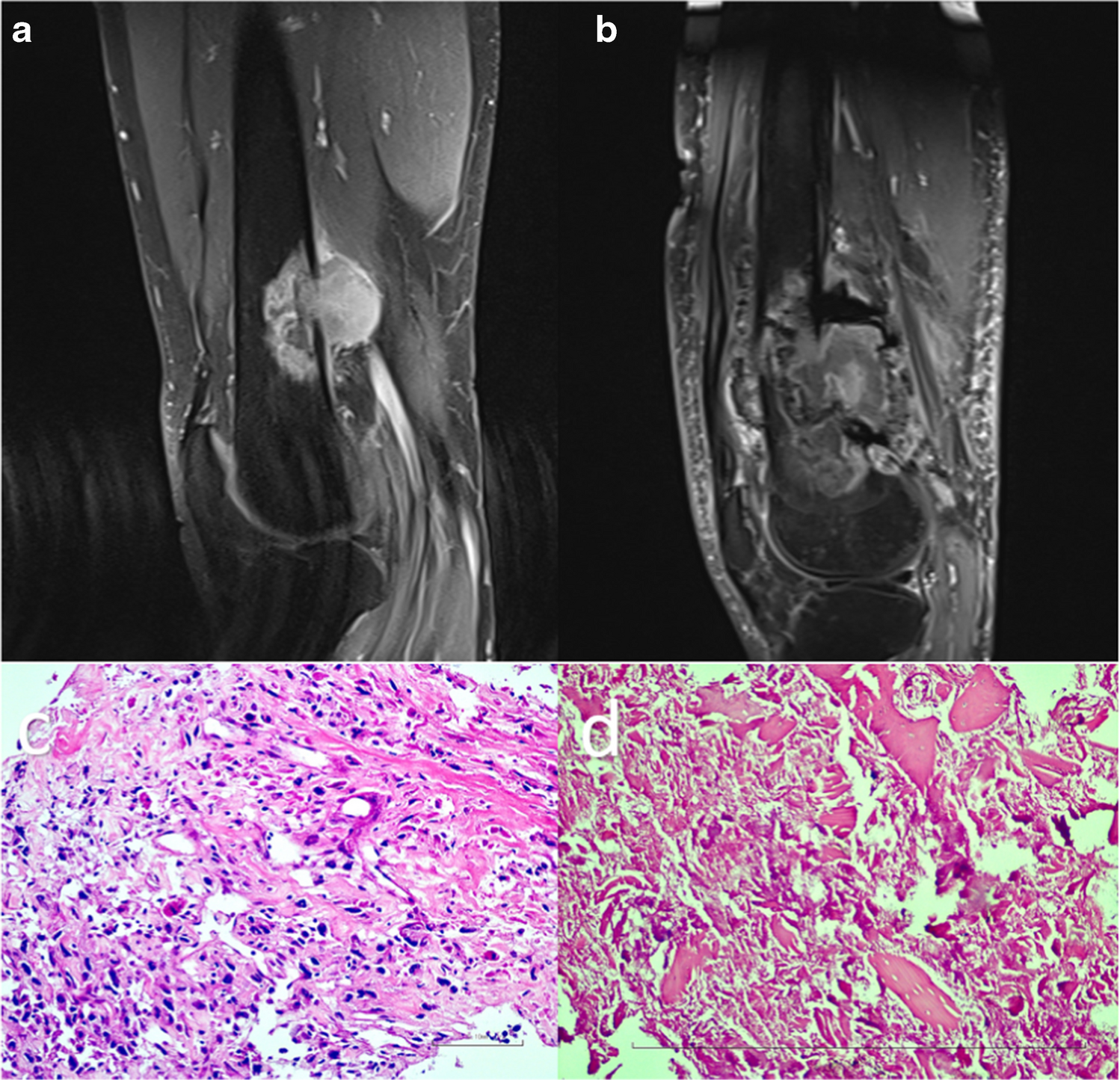
Chondroid lipomaChondroid lipomas are rare, benign, slow-growing adipocytic tumors that most often present in women during the third to fourth decades of life [26]. They typically arise in the extremities or limb girdles and are histologically characterized by nests of lipoblasts embedded within a myxoid or hyalinized chondroid matrix, interspersed with variable amounts of mature fat [26]. On MRI, these lesions appear as well-defined, lobulated masses with areas of T2-hyperintense, fluid-like signal and show variable postcontrast enhancement (Fig. 6) [27, 28]. Radiographs may occasionally reveal internal calcifications. Because chondroid lipomas can mimic myxoid liposarcoma or extraskeletal myxoid chondrosarcoma on imaging, histopathologic confirmation, either by image-guided biopsy or excisional sampling is recommended to establish a definitive diagnosis and guide appropriate management [29].
Fig. 6
Chondroid lipoma in a 51-year-old woman presenting with a slow-growing thigh mass. Axial (A) and sagittal (E) T1-weighted MR images show a well-defined heterogeneous lesion with overall low signal intensity and a small hyperintense focus indicating intralesional fat (arrows). Axial (B) and coronal (D) fat-suppressed T2-weighted images reveal lobulated areas of high signal consistent with a myxoid–chondroid matrix. (C) Axial post-contrast fat-saturated T1-weighted image demonstrates heterogeneous enhancement throughout the lesion. (G) Gross specimen exhibits a gelatinous, lobulated cut surface reflecting the myxoid components.(H) Photomicrograph (H&E, × 200) demonstrates mature adipocytes (*) and multivacuolated lipoblast-like cells embedded within a chondromyxoid matrix (C). Although the imaging appearance may mimic myxoid liposarcoma or extraskeletal myxoid chondrosarcoma, the absence of aggressive imaging features and the histologic demonstration of a chondromyxoid matrix without true cartilaginous differentiation support the diagnosis of chondroid lipoma
AngiolipomaAngiolipomas are benign, encapsulated subcutaneous tumors composed of mature adipocytes interspersed with small, thin-walled blood vessels. These proliferated capillaries commonly exhibit characteristic fibrin microthrombi and predominate at the tumor periphery [19]. Angiolipomas most commonly present as small, often multifocal, tender nodules in adolescents and young adults, particularly along the forearm, but are rare in children [30]. Clinically, patients frequently report pain on palpation. Ultrasonography is the modality of choice for initial evaluation, typically revealing an ovoid, heterogeneous, hyperechoic mass with internal vascularity on Doppler imaging, features that reliably distinguish angiolipoma from the more homogeneous, isoechoic, spindle-shaped lipoma, which lacks intrinsic blood flow [31, 32]. On CT and MRI, angiolipomas appear as fat-containing lesions “dirtied” by their vascular channels; postcontrast studies characteristically demonstrate enhancement of the nonadipose components, permitting a confident imaging diagnosis when correlated with clinical presentation [30].
HibernomaHibernomas are rare, benign soft-tissue neoplasms composed of brown fat cells, most often presenting in adults during the third to fifth decades of life and arising predominantly in the proximal thigh, shoulder, back, or neck [19]. Four histologic variants are recognized: typical (the most common), lipoma-like, myxoid, and spindle cell, each defined by the relative proportion of multivacuolated brown fat cells, univacuolated adipocytes, myxoid stroma, or spindle cell elements. On MRI, hibernomas appear as well-circumscribed, fat-containing masses with signal intensity slightly lower than subcutaneous fat on T1-weighted sequences and incomplete suppression on STIR or fat-saturated T2-weighted images (Fig. 7). Internal thin septations and prominent serpentine or branching vessels producing flow voids are characteristic. However, in some cases hibernomas may mimic atypical lipomatous tumors, and histopathologic confirmation is then required for definitive diagnosis. As a result of their active role in thermogenesis, hibernomas usually demonstrate markedly increased FDG uptake on PET [33,34,35]. Because hibernomas are benign and do not metastasize, complete surgical excision with negative margins is curative. Local recurrence is exceedingly rare and almost always attributable to incomplete resection, underscoring the importance of a thorough surgical approach [36].
Fig. 7
Intramuscular hibernoma in a 35-year-old woman. (A, B) Axial and (C) coronal T2-weighted MR images reveal a well-defined mass within the left paravertebral musculature that is slightly hypointense compared with subcutaneous fat (arrows). (B) Axial fat-suppressed, post-contrast T1-weighted image shows heterogeneous enhancement. (D) Gross specimen photograph demonstrates the characteristic yellow–brown cut surface with prominent central vessels. (E) Photomicrograph (H&E, × 200) displays polygonal eosinophilic “brown fat” cells with granular cytoplasm intermixed with univacuolated adipocytes, confirming hibernoma
MyolipomaMyolipoma is a rare benign neoplasm composed of mature adipose tissue and smooth muscle cells, with a strong female predominance and peak incidence in the fifth to sixth decades of life [19]. Most lesions arise in the abdominal cavity, retroperitoneum, or inguinal regions, although cases in the trunk, extremities, and subcutaneous tissues have been reported [5, 14]. Due to their deep location, tumors are usually large at presentation, often encapsulated, and range from 10–25 cm in size [14].
At gross pathologic examination, these large tumors are usually completely or at least partially encapsulated with a yellow to white appearance. Histologically, myolipomas demonstrate an admixture of smooth muscle and adipose tissue, typically with smooth muscle predominance (2:1), imparting a characteristic “sieve-like” appearance. Immunohistochemistry confirms strong positivity for smooth muscle actin and desmin [14, 19].
On imaging, myolipomas are heterogeneous, reflecting intermixed fat and soft-tissue components. The adipose tissue appears as high T1 and T2 signal that suppresses with fat saturation, whereas the smooth muscle components demonstrate intermediate T1 and intermediate-to-high T2 signal intensity, sometimes with coarse calcifications [5, 14]. Because of these nonspecific features, differentiation from well-differentiated liposarcoma is often not possible on imaging alone [14, 17]. Complete surgical excision is curative, and no cases of recurrence, metastasis, or malignant transformation have been reported [14, 19].
Spindle cell/pleomorphic lipomaSpindle cell/pleomorphic lipoma is a benign adipocytic neoplasm that typically arises in middle-aged to older adults, with a strong male predominance. It most commonly involves the posterior neck, shoulder, and upper back, although lesions may also occur in the trunk and extremities. In the 2020 WHO classification, spindle cell lipoma and pleomorphic lipoma are regarded as part of a single disease spectrum, reflecting shared histologic, genetic, and clinical features [19].
Histologically, these tumors are characterized by a variable admixture of mature adipocytes, bland spindle cells arranged in short fascicles or a “school-of-fish” pattern, rope-like collagen bundles, and, in pleomorphic variants, multinucleated floret-like giant cells. Despite their pleomorphic appearance, mitotic activity is minimal and biologic behavior is indolent. Recurrent deletions involving chromosomes 13q and/or 16q are characteristic, and immunohistochemistry typically demonstrates CD34 positivity, with absence of MDM2 and CDK4 amplification, helping to distinguish these lesions from atypical lipomatous tumor/well-differentiated liposarcoma [19, 23, 37].
On MRI, spindle cell/pleomorphic lipomas often demonstrate variable fat content, resulting in a heterogeneous appearance that may deviate from that of a conventional lipoma. Non-adipose components commonly appear isointense to muscle on T1-weighted images and show variable signal intensity on T2-weighted sequences, depending on the relative proportions of spindle cells, collagen, and myxoid stroma. Contrast-enhanced MRI typically reveals mild to moderate enhancement of the non-fatty componentes (Fig. 8). These imaging features can closely mimic atypical lipomatous tumor, particularly when thickened septa or nodular non-adipose areas are present, representing a frequent diagnostic pitfall.
Fig. 8
Spindle cell/pleomorphic lipoma of the right forearm. Axial T1-weighted image (A) shows a well-circumscribed intermuscular mass in the anterolateral region, with heterogeneous signal intensity, predominantly fatty, and containing non-adipose components. Axial fat-suppressed T2-weighted (B) and coronal post-contrast fat-suppressed T1-weighted (C) images demonstrate suppression of the fatty areas and relative T2 hyperintensity of the non-adipose component, which shows post-contrast enhancement. Although this appearance may mimic atypical lipomatous tumor, the typical anatomic distribution, limited lesion size, absence of thick septa or nodular soft-tissue components, and benign histologic features favor the diagnosis of spindle cell/pleomorphic lipoma
Recognition of the typical anatomic distribution, limited lesion size, and lack of aggressive imaging features, such as infiltrative margins, large nodular soft-tissue components, or marked enhancement, may suggest the diagnosis. However, due to substantial overlap with other adipocytic neoplasms, imaging findings alone are insufficient for definitive characterization, and histopathologic confirmation is often required. Complete local excision is curative, and recurrence is uncommon, with no metastatic potential reported.
Atypical spindle cell/pleomorphic lipomatous tumorAtypical spindle cell/pleomorphic lipomatous tumor (ASPLT) is a recently recognized benign adipocytic neoplasm included in the 2020 WHO classification [19]. It was previously named spindle cell liposarcoma and considered a rare subtype of well-differentiated liposarcoma/atypical lipomatous tumor. However, it has become clear that it is genetically distinct from these neoplasms, lacking the characteristic amplification of MDM2, and that it poses no known risk of dedifferentiation [19, 23]. It typically occurs in middle-aged adults with a slight male predominance and most commonly involves the extremities, limb girdles, or trunk.
Histologically, ASPLTs are composed of variable proportions of bland to mildly atypical spindle cells, pleomorphic multinucleated giant cells, mature adipocytes, and scattered lipoblasts within a fibrous to myxoid stroma [14, 18]. The spindle cells tend to be oriented in bundles, similar to low-grade fibrosarcoma, or have an appearance reminiscent of neural neoplasia. These features help differentiate it from ALT/WDLPS, in addition to the absence of immunohistochemical coexpression of MDM2 and CDK4 and the frequent CD34 positivity [19, 23, 37].
On MRI, these tumors usually appear as poorly circumscribed, heterogeneous masses with intermixed fat and nonadipose components. Signal intensity is variable, reflecting the fibrous, myxoid, and lipomatous elements, with mild to moderate enhancement after contrast. Because of overlapping features with other adipocytic tumors, imaging findings alone are not diagnostic [17].
Despite their atypical histology, ASPLTs follow an indolent clinical course. Complete surgical excision is the treatment of choice, with local recurrence possible but no metastasis described [19].
Lipoma arborescensLipoma arborescens is a distinctive, nonneoplastic process characterized by frondlike proliferation of mature adipocytes within the synovial subintimal connective tissue, most frequently involving the suprapatellar recess of the knee. Although its precise etiology remains unclear, it is not listed in the WHO classification of neoplasms [19], and it is now regarded as a reactive phenomenon linked to chronic joint irritation — commonly seen in degenerative osteoarthritis, rheumatoid arthritis, or after prior trauma [38, 39]. Histologically, the synovium’s subintimal layer is replaced by lobules of mature fat cells, imparting a villous or “tree‐like” appearance [40]. On MRI, lipoma arborescens presents as a frondiform mass of high T1 and T2 signal that suppresses on fat‐saturated sequences, often accompanied by joint effusion and synovial hypertrophy (Fig. 9). These characteristic imaging features, together with its predilection for the suprapatellar pouch, allow for confident, noninvasive diagnosis. Arthroscopic synovectomy or open excision of the fatty villi provides both symptom relief and definitive treatment, with low rates of recurrence.
Fig. 9
Lipoma arborescens in a 26-year-old man presenting with a swollen knee. (A–C) Sagittal T1 (A), sagittal T2 fat-suppressed (B), and sagittal T1 fat-suppressed postcontrast (C) images; and (D, E) axial T2 fat-suppressed (D) and axial T1 fat-suppressed postcontrast (E) images demonstrate frondlike synovial villi within the suprapatellar bursa (arrows), all exhibiting signal intensity identical to that of subcutaneous fat. (F) Gross specimen of resected synovium shows yellow, villous projections consistent with fatty infiltration. (G) Photomicrograph (H&E, × 100) reveals hypertrophied synovial villi with a central core of mature adipose tissue, confirming
Comments (0)