
Remember me

This study was approved by our Institutional Review Board (IRB) and performed in compliance with Health Insurance Portability and Accountability (HIPAA) regulations, with a waiver for written informed consent.
A retrospective search of the electronic medical record database was performed using Illuminate (Softek Illuminate) to identify pediatric patients (< 18 years old) who underwent knee MRI and treatment for LFC OCD lesions in the past 7 years (January 1, 2018–February 28, 2025) at our tertiary free-standing pediatric hospital. For patients with multiple MRI examinations of the same knee, only one examination was included, either the first examination for those managed conservatively or the immediate pre-treatment MRI for those who underwent arthroscopic treatment.
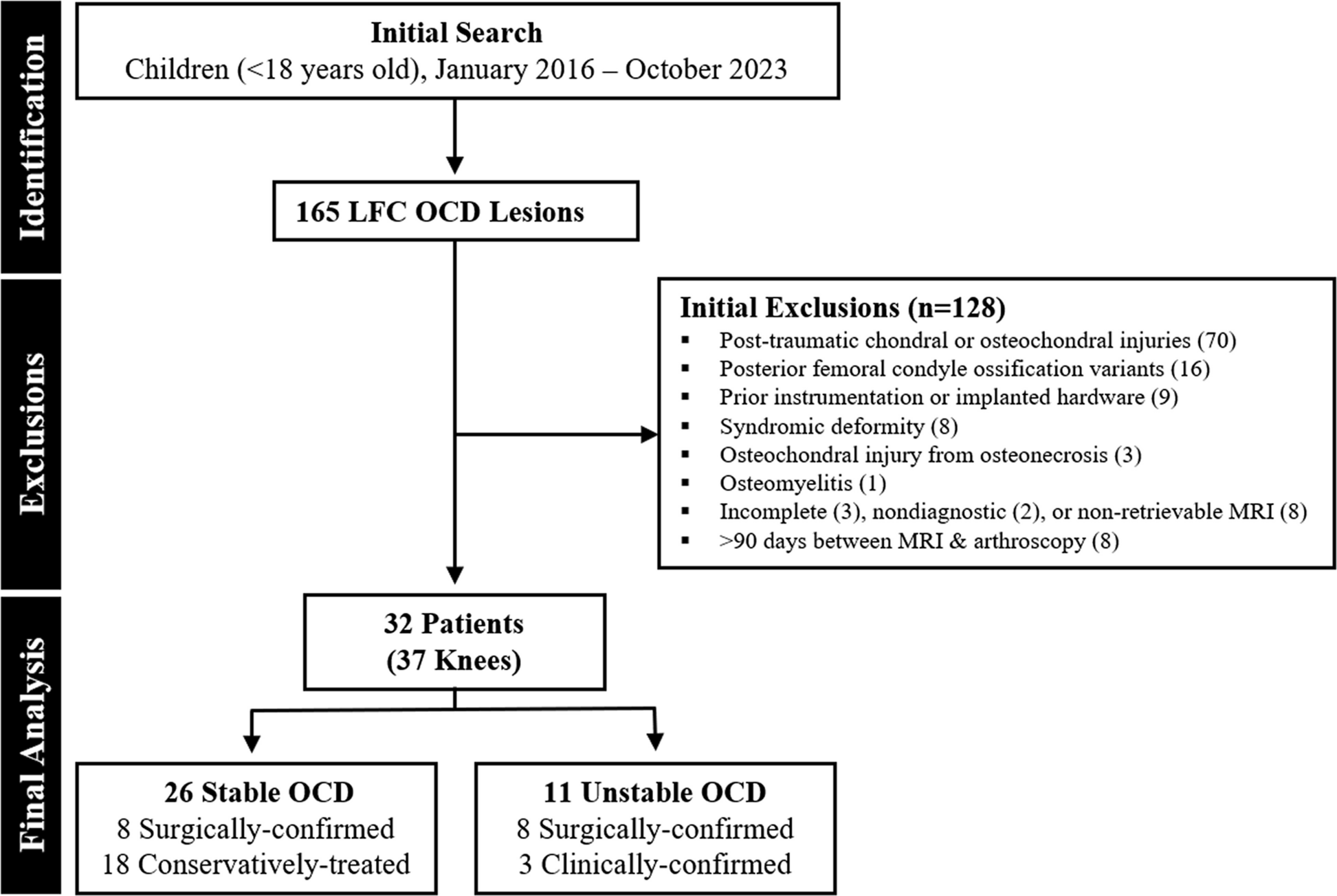
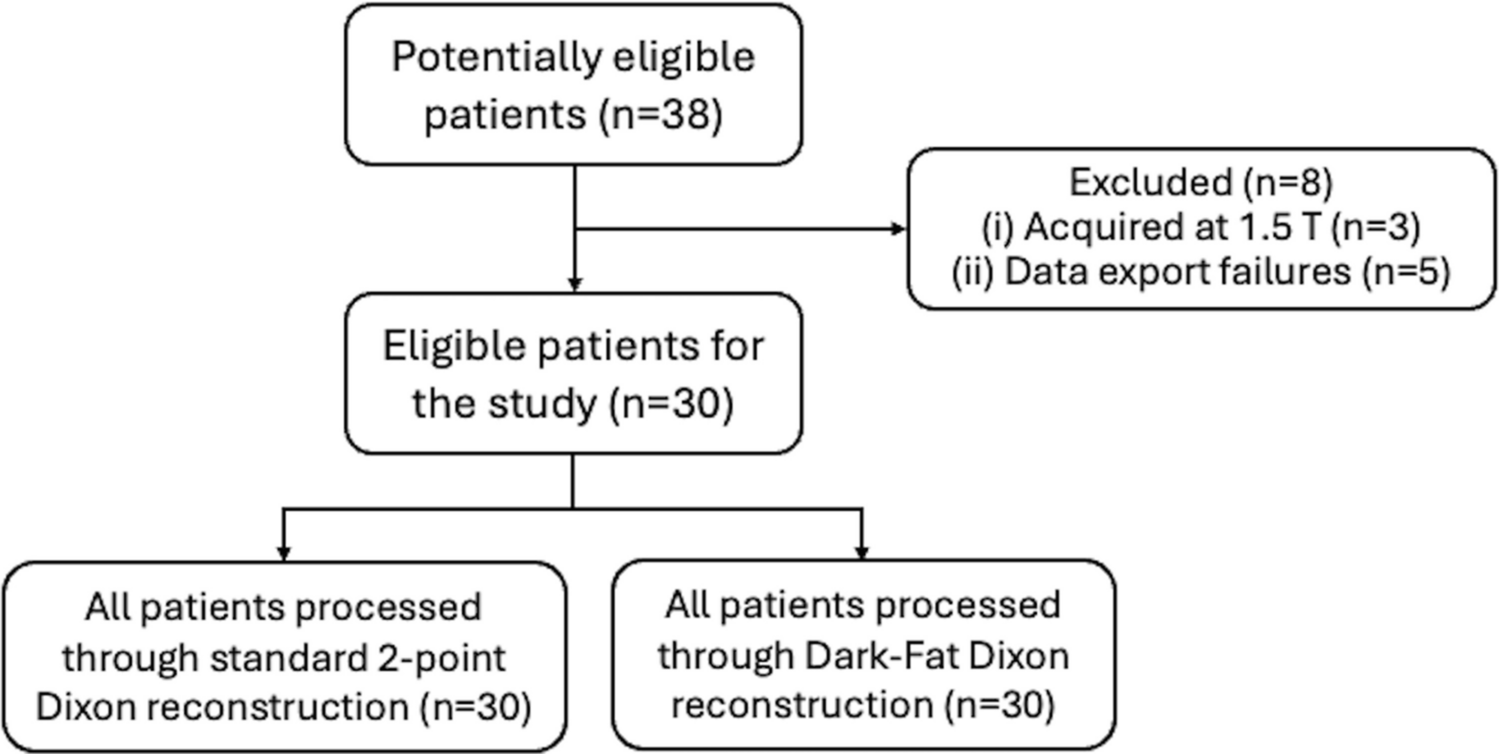
Knee MRI examinations performed following acute traumatic injury or for post-traumatic chondral or osteochondral injuries (n = 70) were excluded. Additionally, examinations on knees with isolated ossification variants (centered over the posterior femoral condyle [20]) (n = 16), prior instrumentation with or without retained hardware (n = 9), from patients with syndromic disorders (n = 8), osteochondral injury from osteonecrosis (n = 3), or osteomyelitis (n = 1) were also excluded. Incomplete (n = 3), nondiagnostic (n = 2), or non-retrievable MRI examinations (n = 8) as well as those with > 90 days between MRI and arthroscopy (n = 8) were also excluded (Fig. 1).
Fig. 1
Flow diagram. Diagram shows patient identification and exclusions, which yielded the final set of lateral femoral condyle (LFC) osteochondritis dissecans (OCD) cases that were included for analysis
MRI techniqueMRI examinations were performed with patients in the supine position and knees in full or near-full extension using either a 1.5-Tesla (Avanto; Siemens Healthineers) or 3-Tesla magnet (Magnetom Prisma and Skyra, Siemens Healthineers) and a 15-channel phased-array knee coil (Tx/Rx coil, Siemens Healthineers, Munich, Germany). The clinical protocol included turbo spin-echo pulse sequences acquired in all 3 orthogonal planes: axial and sagittal T2-weighted fat-suppressed (TR/TE = 4500–5500 ms/45–65 ms); sagittal intermediate-weighted (non-fat-suppressed) and coronal intermediate-weighted fat-suppressed (TR/TE = 3000–4000 ms/25–40 ms); and coronal T1-weighted pulse sequences (TR/TE = 500–650 ms/10–20 ms). The field of view was 14–16 cm, the matrix size ranged between 384 × 384 and 512 × 512, and slice thickness was 3 mm with an inter-slice gap ranged between 0 and 10%.
Review of MRI examinationBlinded to outcome, all MRI examinations were retrospectively reviewed by two board-certified, fellowship-trained radiologists—one in pediatric and musculoskeletal radiology (JCN, with 12 years of post-fellowship clinical experience) and the other in pediatric radiology with a focus in musculoskeletal imaging (LG, with 5 years of post-fellowship clinical experience). Disagreements from independent reviews were resolved through a separate consensus review.
Examinations were assessed for the presence of a knee joint effusion, regional skeletal maturity, various direct and indirect findings that can associate with lesion instability [8]. Joint effusion was characterized by the presence of hyperintense signal intensity on fluid-sensitive images that distended both medial and lateral suprapatellar gutters. Skeletal maturity was based on the patency of the distal femoral and proximal tibial growth plates. Using coronal and sagittal images, the knee was classified as immature if both growth plates were open (a uniform band of growth plate signal intensity that is hypointense on T1-weighted and hyperintense on fluid-sensitive pulse sequences). The knee was classified as maturing if there was narrowing, indistinctness, or loss of this growth plate signal that involved at least 25% of the proximal tibial growth plate, or mature if there was complete or near-complete closure of the proximal tibial growth plate and > 75% loss of the distal femur growth plate. Due to the relatively smaller sample size, skeletally maturing and mature knees were grouped and compared with skeletally immature knees.
Direct findings of lesion instability include an osteochondral defect, intraarticular bodies, cartilage alteration, and bone plate disruption. An osteochondral defect (or “empty crater”) resulted from a displaced progeny, leaving behind a fluid-filled concavity at the articular surface [1]. Intraarticular bodies were defined as detached chondral or osteochondral fragments. Cartilage alteration included full-thickness cartilage fissure or disruption (a band of high signal intensity) and dark cartilage lesions (or “omen sign,” a band of low signal intensity) [20,21,22,23,24,25] (Fig. 2). If cartilage alteration was detected, the quantity (single or multiple) and the location (anterior, posterior, medial, or lateral) were also recorded. Among skeletally maturing and mature patients, the subchondral bone plate is located beneath the articular cartilage and its disruption can be focal (defined as ≤ 3) or multifocal (defined as > 3 foci of disruption) [22], whereas among skeletally immature patients, the ossification front is located beneath the chondroepiphysis, which can be normally located or receded, reflecting localized endochondral ossification dysfunction [26].
Fig. 2
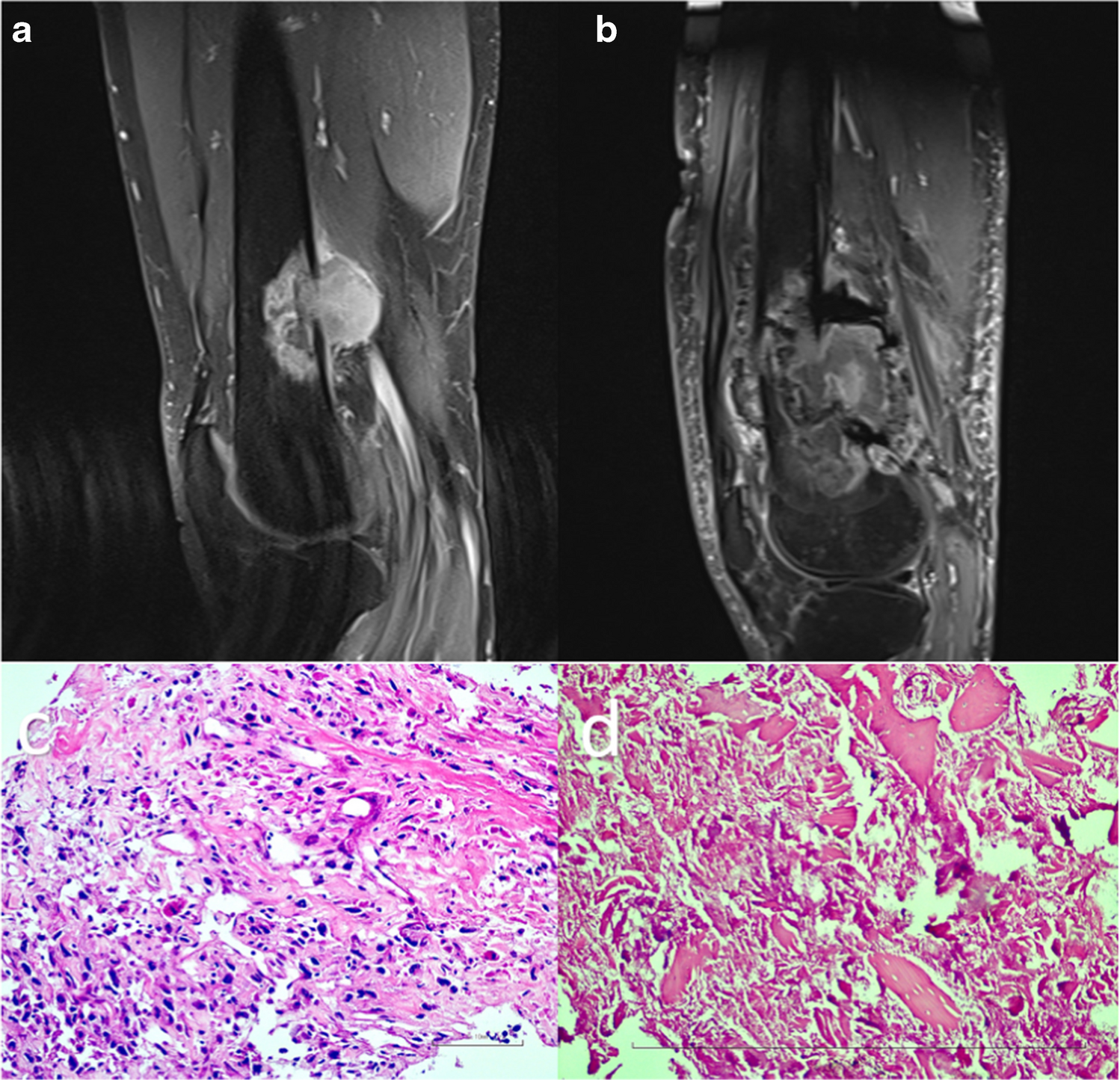
Unstable LFC OCD lesion in a 17-year-old skeletally mature female. Sagittal T2-weighted fat-suppressed (A) and coronal intermediate-weighted fat-suppressed (B) MR images show a partially detached progeny with a fluid-signal intensity progeny-parent bone interface (arrowheads). Note the intra-articular body posteriorly (triangle) and a torn, anteriorly shifted and laterally extruded discoid lateral meniscus (arrows). These findings were confirmed during arthroscopy.
Indirect findings of lesion instability include the presence of a progeny-parent bone interface, cysts, altered articular surface curvature, parent bone marginal rim, and perilesional marrow edema. Interface was defined as a discrete separation between the progeny and the parent bone. If present, the extent (minimal, < 25%; moderate, 25–75%; or extensive, > 75%) and signal intensity (intermediate or fluid-high on T2-weighted images) of the interface were also recorded [21,22,23]. Cysts were defined as round foci with overall high signal intensity that are centered at the interface. If present, the total number and the diameter of the largest cyst were recorded [21,22,23] (Fig. 3). Articular surface curvature was categorized as maintained or altered, and the latter can convex or concave surface morphology [1]. Parent bone marginal rim was defined as a marginal band of low signal intensity on T2-weighted images [27]. If present, the extent (minimal, < 25%; moderate, 25–75%; or extensive, > 75%) of the rim was recorded. Perilesional marrow edema (low signal intensity on T1-weighted images and high signal intensity on fluid-sensitive images) was similarly subcategorized into mild (< 25%), moderate (25–75%), or extensive (> 75%) based on the extent of its craniocaudal involvement of the LFC (Fig. 4). For completeness, lesion volume is calculated using the ellipsoid formula (length × width × depth × 0.5) [28] and 3 dimensions of the lesion were measured by a research student (CY) with over 2 years of musculoskeletal research experience and under the supervision of the pediatric musculoskeletal radiologist (JCN).
Fig. 3
Unstable LFC OCD lesion in a 15-year-old skeletally immature male. Sagittal T2-weighted fat-suppressed (A) and intermediate-weighted (B) MR images show an intermediate signal intensity progeny-parent bone interface (arrowhead, A) that is defined by the underlying parent bone marginal rim. At the anterior margin of the OCD lesion, there is a 4.5-mm cyst (dashed arrow) that underlies a hyperintense cartilage fissure (chevron). A ballotable unstable OCD lesion was confirmed at arthroscopy.
Fig. 4
Unstable LFC OCD lesion in a 15-year-old skeletally immature male. Sagittal T2-weighted fat-suppressed MR image shows an abnormal convex surface contour (arrow), multiple cysts (triangles, largest measured 7 mm, not shown), parent bone marginal rim (block arrow), and extensive perilesional marrow edema (bracket). A protuberant unstable OCD lesion was confirmed at arthroscopy with overlying cartilage loss.
Clinical data and reference standards for OCD stabilityThe electronic medical records were reviewed to collect demographic and clinical information including age at the time of the MRI examination, laterality of the involved knee, duration of symptoms, BMI percentile (within 6 months of the MRI), lesion stability, and if available, operative findings. BMI was determined using the patient’s weight and height, which was then converted to percentile classification based on age- and sex-matched children from the CDC growth charts [29]. BMI percentile was classified as underweight if < 5%, normal weight if between 5 and < 85%, or as overweight or obese (hereafter, overweight/obese) if ≥ 85% [30]. For patients with bilateral lesions, the time interval between diagnoses was recorded. For lesions that underwent arthroscopy, the time interval between MRI and arthroscopy was recorded and for lesions that underwent conservative treatment, the time interval between initial MRI and latest follow-up was recorded.
Each LFC OCD lesion was classified as stable or unstable. For those patients who underwent arthroscopy, a LFC OCD lesion was considered unstable if the overlying cartilage was disrupted or if the lesion was ballotable upon probing [1, 22]. For those patients who underwent conservative management, a LFC OCD lesion was considered stable if symptoms improved or resolved, and follow-up imaging showed reduced lesion size, less conspicuous progeny, resolving and/or resolved parent bone marginal sclerosis on follow-up knee radiographs, reduced and/or resolved progeny-parent-bone interface, and/or cyst(s) on follow-up MRI examinations [20, 31,32,33,34,35,36] (Fig. 5).
Fig. 5
Conservatively treated LFC OCD lesion in a 13-year-old skeletally immature male. Anteroposterior (A, C) and lateral (B, D) radiographs at initial presentation (A, B) and 2 years later (C, D) show a less conspicuous progeny (brackets, A-B), no progeny-parent bone interface, or development of parent bone marginal sclerosis. Patient reported resolved symptoms.
Statistical analysisAll statistical analyses were performed using R and R Studio (Version 1.1.423; R Foundation for Statistical Computing). A P-value < .05 was considered statistically significant. Interrater agreement for various MRI findings was evaluated using the Cohen’s kappa (k) with agreement categorized as slight (≤ .20), fair (.21–.40), moderate (.41–.60), substantial (.61–.80), almost perfect (≥ .81), and perfect (1.00) [37].
The Shapiro–Wilk test was used to assess the distribution of the variables. Continuous variables, if normally distributed, were reported as means and standard deviations (SD) and if not, reported as medians and interquartile ranges (IQR). Categorical variables were summarized using counts and percentages.
Comparisons between stable and unstable lesions were performed using the independent sample t, Mann–Whitney U, or the Fisher exact tests, depending on the distribution of data and sample size. Although univariable logistic regression analyses were performed to evaluate the utility of demographic and MRI findings for distinguishing lesion stability, the relatively small sample size compromised the reliability estimates for the multivariable logistic regression analysis increased the risk of model overfitting. Instead, the receiver operating characteristic (ROC) curve analysis provided a more robust and interpretable means of assessing the diagnostic performance of individual predictors while avoiding the assumptions and limitations of multivariable modeling in underpowered datasets. The area under the curve (AUC) was used as a summary measure of discriminative ability.
Comments (0)