Enteral nutrition-associated esophageal bezoars are rare but clinically significant complications, often linked to casein-containing formulas that solidify in acidic environments [3,4,5,6,7]. In this case, the enteral formula used (Termeal series) contained casein, consistent with previous studies. The in vitro experiment performed in this study provides mechanistic support for the formation of casein-based esophageal bezoars under highly acidic conditions. When the casein-based enteral formula was exposed to simulated gastric juice (hydrochloric acid–adjusted saline, pH 1.0, without pepsin), rapid and reproducible solidification occurred, whereas the formula remained liquid when mixed with solutions at pH 2.0–5.5. These findings suggest that extreme acidity alone, even in the absence of digestive enzymes such as pepsin, is sufficient to induce coagulation of casein-based formulas. This observation is consistent with the known physicochemical properties of casein micelles, which destabilize and aggregate at very low pH levels [8, 9], whereas peptide-based or whey-dominant products remain in solution, even under strong acidity.
It should be emphasized that this patient was receiving proton pump inhibitor therapy, making sustained exposure to strongly acidic gastric juice unlikely. However, intragastric pH under acid-suppressive therapy is not uniform and may fluctuate, particularly in the early postoperative period. Moreover, local physicochemical conditions within the esophagus, such as prolonged stasis of enteral formula, concentration due to dehydration, and limited clearance, may facilitate coagulation of casein-containing formulas even without continuous exposure to extreme acidity. Notably, our in vitro experiment demonstrated that solidification of the casein-based formula occurred rapidly upon exposure to a strongly acidic environment. This finding raises the possibility that even brief or transient exposure to localized acidic conditions, despite ongoing proton pump inhibitor therapy, could act as a trigger for coagulation of the enteral formula when it is retained within the esophagus.
Unlike cases involving elderly ICU patients with prolonged tube feeding and multiple comorbidities, our patient was a young postoperative individual who developed a bezoar within a relatively short duration of enteral nutrition. This highlights that even short-term administration of a casein-containing formula, if combined with postoperative esophageal stasis and reflux, can predispose patients to bezoar formation. Our findings suggest that the risk of bezoar development is not solely dependent on prolonged feeding duration or intrinsic esophageal motility disorders, but may also arise from brief episodes of postoperative stasis combined with exposure to highly acidic gastric juice. Consequently, careful selection of enteral formulas should be considered in postoperative or critically ill patients at risk of esophageal reflux and impaired clearance.
In addition to impaired esophageal peristalsis, nasogastric tubes may contribute to bezoar formation by promoting gastroesophageal reflux and facilitating pooling of enteral formula within the esophageal lumen [10, 11]. Several earlier reports have associated enteral formula bezoars with achalasia, systemic sclerosis, Guillain–Barré syndrome, and myasthenia gravis, all of which reduce esophageal clearance [12]. Our patient had no intrinsic motility disorder; however, prolonged supine positioning, repeated intubation, and postoperative dysphagia likely created sufficient stasis for casein-containing formula coagulation.
Medications commonly administered in intensive care settings, including opioids, sedatives, and certain antacids, may delay gastric emptying or contribute to bezoar formation [13]. Historical cases involved the use of sucralfate- or aluminum-based antacids, both of which have binding properties that facilitate concretion [4, 7, 12]. In our case, such agents were not administered; however, fentanyl and sedative medications were used for respiratory support, which may have diminished swallowing frequency and delayed esophageal clearance. Thus, although the medication profile differed from that of the earlier cases, the degree of pharmacological contribution could not be excluded.
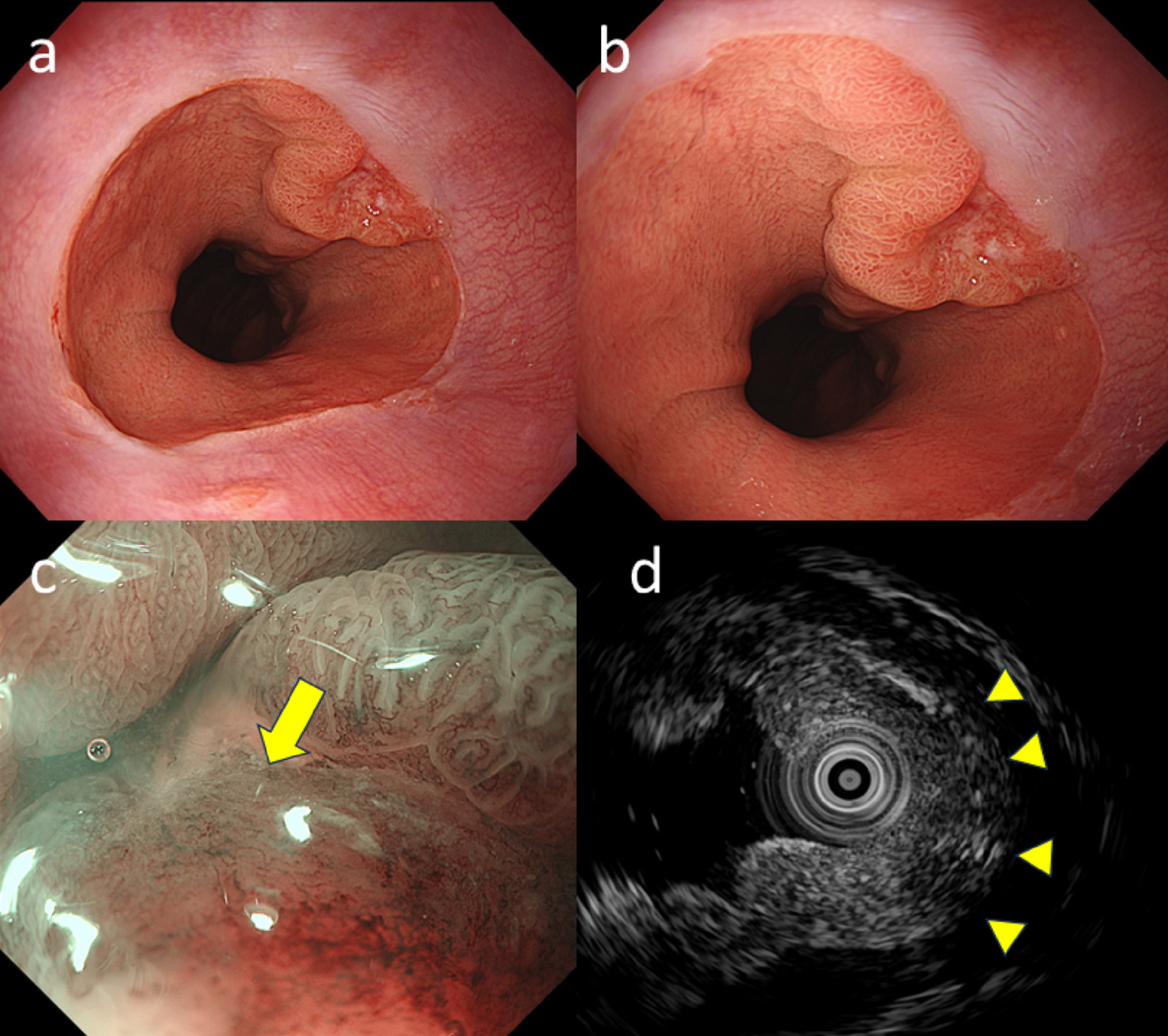
Management strategies for casein-induced bezoars vary. Successful dissolution has been reported using pancreatic enzyme preparations, effervescent drinks, or prolonged lavage with bicarbonate-containing solutions [3, 4, 12]. Endoscopic fragmentation remains the most commonly employed method, although it is technically demanding and occasionally requires multiple sessions [12]. Rare cases of esophageal perforation after aggressive manipulation emphasize the need for caution [14]. Presently, the bezoar was only partially fragmented with forceps and suction; however, the degree of fragmentation was limited, and most of the mass was ultimately dislodged into the stomach for removal.
Preventive measures include semi-recumbent feeding to reduce reflux, routine flushing of feeding tubes, acid-suppressive therapy, prokinetics, and the selection of non-casein formulas for high-risk patients [3, 4]. Potassium-competitive acid blockers (P-CABs) provide more rapid and potent gastric acid suppression than conventional proton pump inhibitors and may more promptly elevate intragastric pH. From a theoretical standpoint, administration of a P-CAB via a nasogastric tube during enteral feeding with casein-based formulas could reduce the likelihood of casein coagulation by minimizing exposure to highly acidic conditions. Although the preventive efficacy of P-CABs for enteral nutrition–associated bezoars has not been systematically evaluated, such an approach may be considered as a potential preventive strategy in postoperative or critically ill patients at high risk for esophageal stasis and reflux. Nasointestinal feeding routes may decrease esophageal exposure to enteral formulas.

Comments (0)