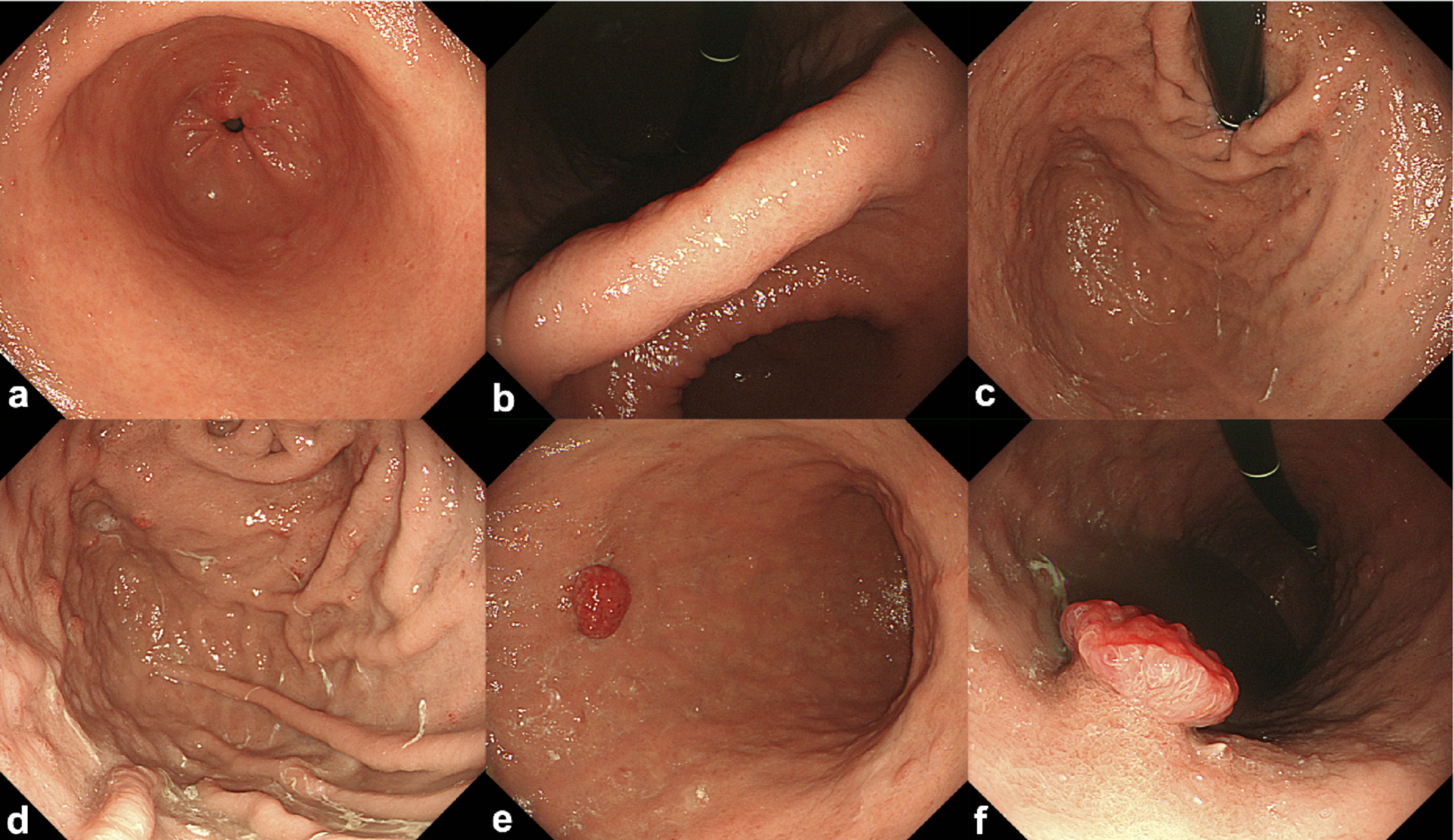
We recently encountered a rare case of a gastric NET exhibiting pedunculated and reddish morphology. Endoscopic examination revealed advanced corpus dominant mucosal atrophy and histopathological analysis of the resected specimen showed ECMs in the deep mucosal layer. Although serum anti-parietal cell and anti-intrinsic factor antibodies were not measured, the combination of endoscopic and histological findings strongly suggested the presence of underlying autoimmune gastritis, meaning Rindi type 1 NET. In this case, the patient was taking proton pump inhibitor (PPI), but the serum gastrin level was 6,300 pg/ml, which is more than 60 times the normal value. Even considering the effect of PPI, this level was abnormally high, suggesting the possibility of autoimmune gastritis.
For Rindi type 1 gastric NETs larger than 10 mm, surgical resection is recommended in Japan [5]; however, in Europe, endoscopic treatment is considered an acceptable option in the absence of muscularis propria invasion [6]. In the present case, ESD was selected after careful consideration of the patient’s general condition. Regarding additional surgical treatment, the Japanese guidelines recommend distal gastrectomy or total gastrectomy with D2 lymph node dissection [5]. Previous reports have shown that antrectomy for Rindi type 1 gastric NETs can correct hypergastrinemia and lead to tumor regression [7]. In this case, taking into account the potential postoperative decline in quality of life in daily living, distal gastrectomy including the antrum was selected. Because there remains a risk of recurrence of NETs in the remnant stomach, regular postoperative endoscopic surveillance was considered necessary.
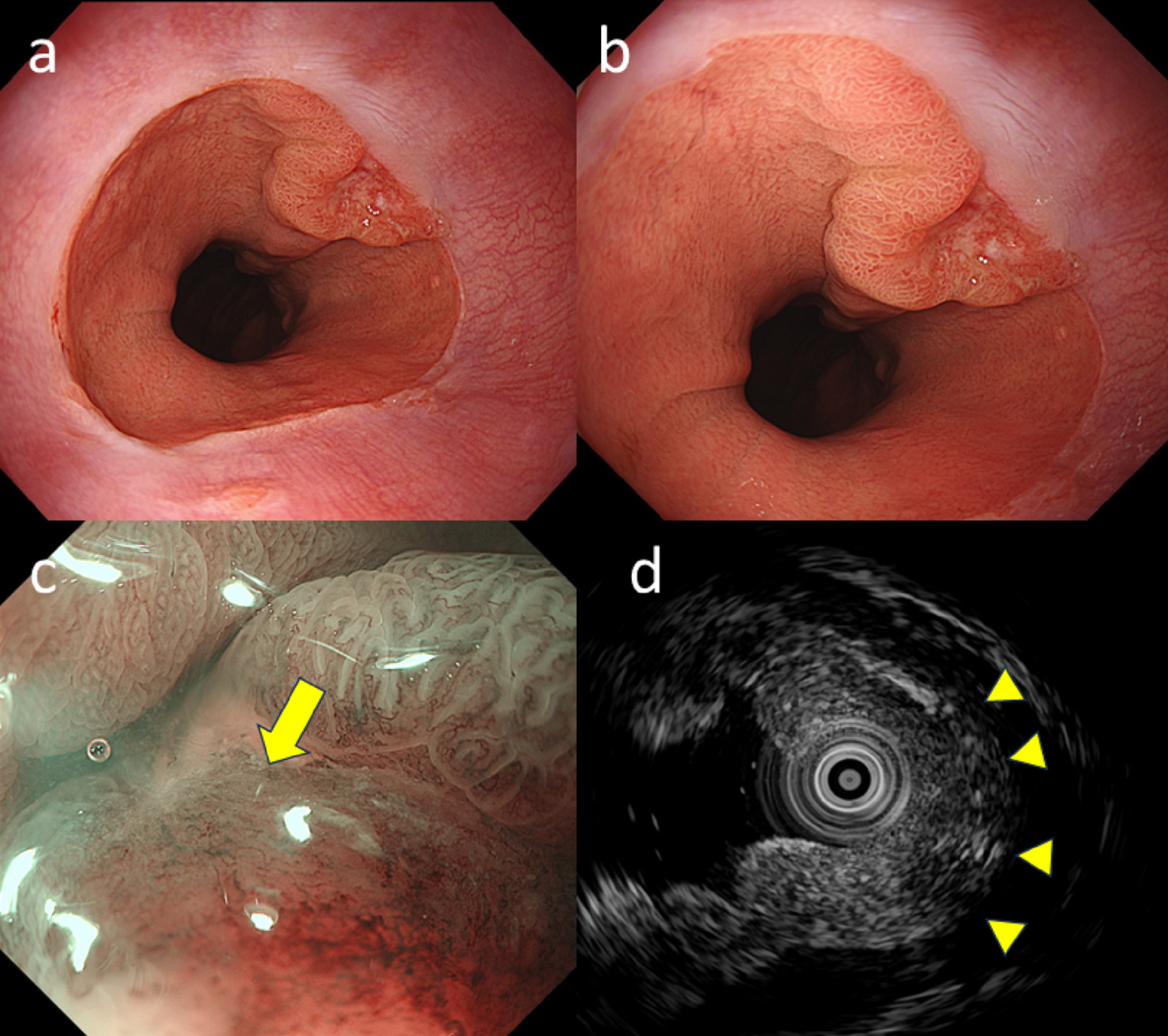
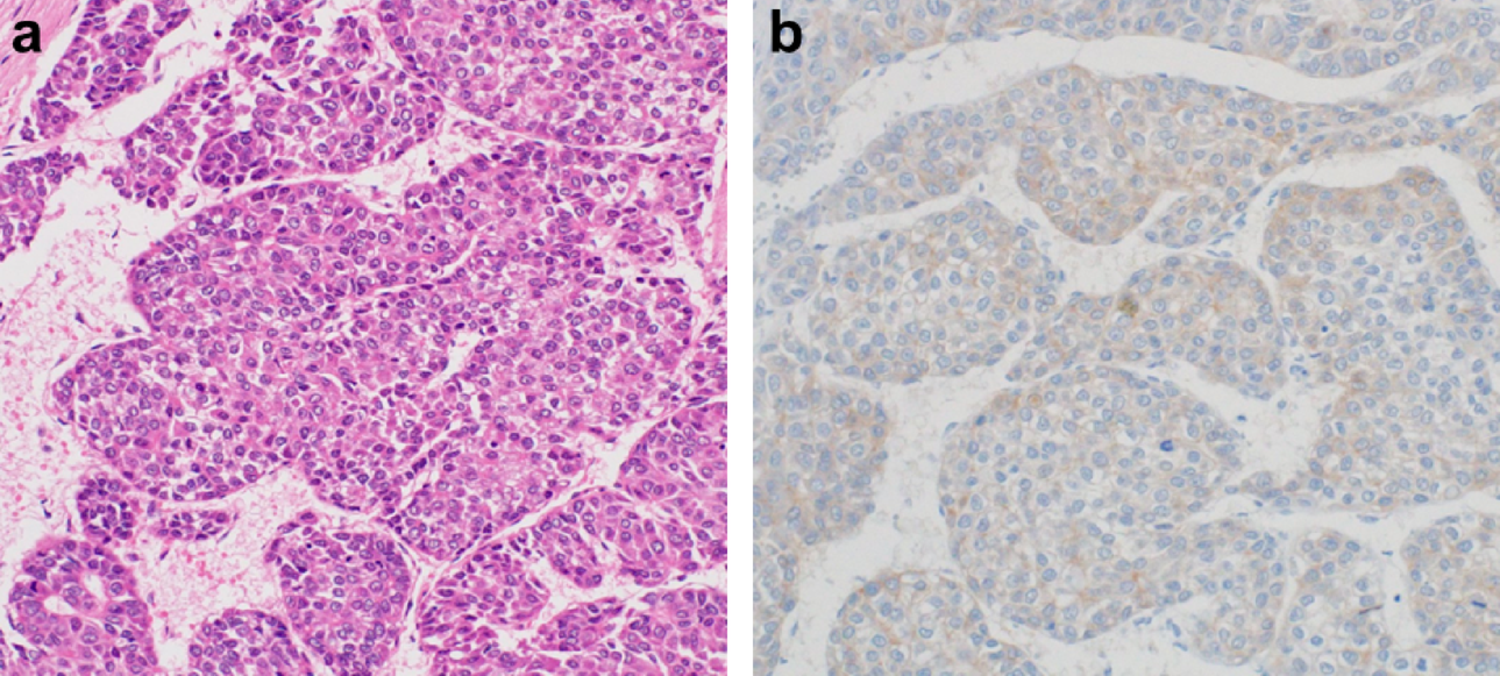
Gastric NETs, which arise from ECL cells, typically expand toward the submucosa and present as SMT-like protrusions under endoscopy [4]. These lesions often appear red or normal in color and may exhibit surface vascular dilation [4]. In this case, vascular dilation was observed, as in typical cases; however, the presence of a pedunculated and reddish morphology, complicating diagnosis based on the usual morphological features of gastric NETs. Endoscopic findings in this case revealed inflammatory changes on the surface of the elevated lesion, characterized by a mixture of redness and whitish coating, without any evidence of tumor exposure on the mucosal surface. In contrast, histopathological evaluation of the resected specimen showed denudation of the surface epithelium with tumor cells exposed at the surface. The denudation of the surface foveolar epithelium may have been caused either by active erosion present at the surface or by an artifact introduced during the resection process.
Although reports of pedunculated gastric NETs are extremely rare, a case report by Takeda et al. described an indistinct boundary between the head and stalk, with the head of the tumor appearing more reddish than the stalk [8]. In the present case, the boundary between the head and neck was also unclear, and similar redness of the head was observed; however, the degree of redness was more pronounced than that reported previously [8]. Histopathological findings of the head showed that the tumor extended and was distributed closer to the surface than in previously reported cases and was accompanied by abundant proliferation of dilated capillaries, which was considered to have resulted in the marked reddish mucosal appearance [8]. Furthermore, while vascular dilation was observed only in the head on NBI in the previously reported case, vascular dilation was observed only in the neck in the present case. Typical vascular dilation in gastric NETs is thought to result from expansive growth of the tumor in the submucosa, leading to stretching of the superficial capillaries [4]. Because no tumor component was present in the superficial layer of the neck in this lesion, it was presumed that the superficial capillaries were stretched in a manner similar to that seen in typical cases, resulting in the observed vascular dilation.
Another report of a pedunculated gastric NET suggested that, in cases where the tumor does not invade the muscularis propria, repeated peristaltic activity may cause gradual separation between the tumor and the underlying muscle layer, ultimately resulting in a pedunculated appearance [9]. In this case, the lesion was located on the greater curvature of the gastric body. Frequent mechanical stimulation due to peristalsis at this site may have contributed to the development of the pedunculated form. In the pathological findings of the resected specimen from this case, the tumor was primarily located within the mucosal layer, and its grossly pedunculated appearance was likely due to this localization. However, the mechanism by which the tumor developed toward the mucosal surface rather than the deeper layers remains unclear. Accumulation of additional similar cases may lead to new insights into this growth pattern in the future.
In conclusion, recognizing that gastric NETs can occasionally exhibit unusual pedunculated and reddish morphology may aid in accurate diagnosis.

Comments (0)