With advances in UC treatment, the number of patients who can be managed long-term without surgery has increased. However, prolonged colonic mucosal inflammation is associated with an increased incidence of UC-associated neoplasia. In addition to neoplastic transformation, LPDs have also been reported in association with immunosuppressive therapy, including immunomodulators such as 6-mercaptopurine and azathioprine, as well as biologic agents such as anti–tumor necrosis factor-α antibodies [10].
A B-cell lymphoma characterized by a small number of malignant RS cells scattered within a background of extensive inflammation and immune cell infiltration, cHL exhibits a bimodal age distribution, with incidence peaks at approximately 20–30 and 50–70 years of age [11]. Among younger individuals, cHL is the most common type of lymphoma; however, it is relatively rare in older adults because of the increased incidence of other lymphoma subtypes, such as diffuse large B-cell, marginal zone, and follicular lymphomas [12]. EBV infection is considered to be causally associated with approximately 25–40% of cHL cases [11, 13]. This disease can also be associated with immunosuppressive conditions and has been reported in patients with human immunodeficiency virus infections and autoimmune diseases [11].
Vedolizumab is a gut-selective monoclonal antibody that binds the α4β7 integrin and inhibits its interaction with mucosal addressin cell adhesion molecule-1 (MAdCAM-1) expressed in gut-associated lymphoid tissues (GALT) and intestinal mucosa [14]. Through this mechanism, vedolizumab selectively antagonizes α4β7-mediated adhesion/extravasation of gut-homing lymphocytes—particularly memory/effector T-cell subsets—and thereby reduces intestinal lymphocyte trafficking without the broader systemic immune effects associated with nonselective α4β7 blockade [15, 16]. While this tissue-selective mechanism underlies its favorable safety profile, emerging human and experimental data suggest that α4β7 blockade may also modulate GALT, potentially attenuating local mucosal immune surveillance [17]. In susceptible hosts, such localized impairment of intestinal immune control could theoretically contribute to inadequate containment of oncogenic viruses such as Epstein–Barr virus. We emphasize that this remains a hypothesis, and causality cannot be inferred from a single case; however, the biology of α4β7–MAdCAM-1 trafficking provides a plausible framework for considering vedolizumab-associated disruption of intestinal immune surveillance as a contributing factor to EBV-associated lymphoma development.
In the present case, EBER in situ hybridization was positive, confirming that the tumor cells were infected with EBV. Immunomodulator therapy was discontinued eight years prior after only two weeks of treatment, and treatment with vedolizumab was initiated 31 months prior to the current presentation. Eighteen months prior, colonoscopy revealed early lesions later considered compatible with incipient cHL. Fifteen months prior, the patient was diagnosed with breast cancer and started aromatase inhibitor therapy, after which lymphoproliferative disease became clinically evident. These findings suggest that pathogenesis may have involved reactivation of latent EBV infection and subsequent proliferation of infected B cells under locally altered intestinal immune conditions associated with vedolizumab therapy. Similarly, a previous report described EBV-related mucosal ulceration occurring during vedolizumab treatment [18]. Vedolizumab selectively suppresses intestinal immune responses by inhibiting lymphocyte trafficking to the gut, which may create an environment prone to the development of focal intestinal immune deficiency and dysregulation-related lymphoma. To the best of our knowledge, this is the first reported case of cHL associated with vedolizumab therapy.
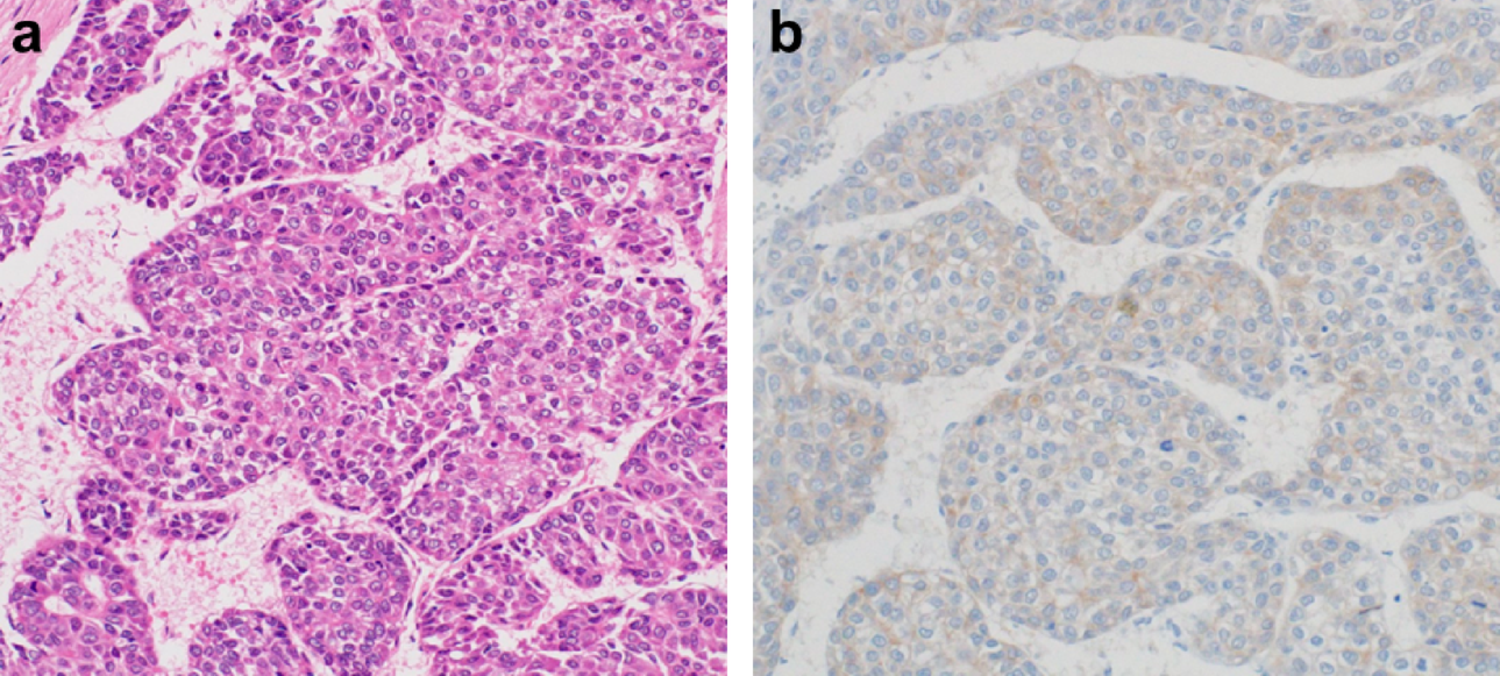
From a pathological perspective, the main differential diagnoses in the present case included EBV-associated mucocutaneous ulcer (EBV-MCU) and EBV-positive diffuse large B-cell lymphoma (DLBCL). According to the WHO Classification of Tumours of Haematolymphoid Tumours, 5th edition, EBV-MCU typically demonstrates broad EBER positivity across a wide spectrum of lymphoid cells of varying sizes [9]. In contrast, in cHL, EBER positivity is usually confined to a limited number of large atypical RS cells. In the present case, EBER in situ hybridization showed positivity restricted to scattered large atypical RS cells, whereas the majority of background cells were EBER-negative, a distribution pattern consistent with cHL rather than EBV-MCU. Furthermore, EBV-positive DLBCL is characterized by diffuse sheet-like proliferation of large atypical B cells. However, such a diffuse growth pattern was not observed in this case; instead, only rare large atypical cells were observed in the lesion. Taken together with the immunophenotypic findings, including CD30 positivity, CD20 expression in RS cells, and high PD-L1 expression, these findings supported the diagnosis of cHL.
Surgical resection may improve the prognosis of patients with localized malignant lymphoma when combined with chemotherapy; however, these findings are primarily based on cases of non-Hodgkin B-cell lymphoma, and the benefits for cHL remain unclear [19, 20]. Surgery alone is generally not considered a curative treatment for cHL, and standard management relies on systemic chemotherapy with or without radiotherapy [21]. In the present case, the sigmoid colon lymphoma was not diagnosed preoperatively. Surgery was considered appropriate because of the presence of high-grade dysplasia in the transverse colon and refractory bleeding, presumably caused by the sigmoid lesion, which did not respond to medical treatment. Other biological agents and immunomodulators that could suppress systemic antitumor immunity were not considered viable options because the patient was undergoing treatment for breast cancer. Ultimately, the patient declined the recommended chemotherapeutic regimen. In elderly patients with comorbidities, including concurrent malignancies, treatment decision-making for cHL often requires careful individualization, balancing potential therapeutic benefit against treatment-related toxicity and patient preference [22]. Although postoperative PET–CT revealed no significant lymph node involvement throughout the body, and the patient has remained recurrence-free for 10 months after surgery alone, this favorable short-term outcome should be interpreted with caution. Careful follow-up is warranted to monitor for potential disease progression.
The present case highlights the complexity of lymphoma development in elderly patients with UC. The occurrence of EBV-associated cHL in this patient should be interpreted within a multifactorial framework rather than being attributed to a single causative factor. Elderly-onset inflammatory bowel disease represents a growing clinical population, and age-related immune dysfunction is increasingly recognized as an important contributor to malignancy risk [23]. Immunosenescence may impair immune surveillance of latent viral infections, thereby facilitating EBV reactivation and lymphomagenesis. In addition, the patient had a history of breast cancer treated with an aromatase inhibitor. Although causal inference cannot be established, previous clinical reports and experimental studies have suggested that estrogen-deprived conditions may influence lymphoid proliferation [24, 25]. Aromatase inhibitor therapy may therefore represent a background factor potentially modulating lymphoma progression. Although the development of lymphoma in this case may have been influenced by multiple factors—including vedolizumab-related alterations in intestinal immunity, age-related immune dysfunction, and aromatase inhibitor therapy—clinicians should remain aware of the potential for intestinal lymphoma to occur during vedolizumab therapy.
In the present case, endoscopic biopsy of the sigmoid lesion performed prior to surgery did not reveal morphologically atypical lymphoid cells and was initially interpreted as granulation tissue. However, retrospective pathological re-evaluation demonstrated the presence of a relatively smaller number of EBER-positive large cells than were identified in the surgical specimen. Routine histological evaluation alone may be insufficient to detect early-stage EBV-associated lymphoma. Therefore, when lymphoma is clinically suspected—particularly in patients with UC receiving biologic agents or immunomodulatory therapy—EBER in situ hybridization should be actively considered, even when initial biopsy specimens lack clear morphological features of malignancy. EBER staining may serve as a valuable adjunctive tool for the early detection of EBV-associated lymphoproliferative disorders and facilitate timely diagnosis.
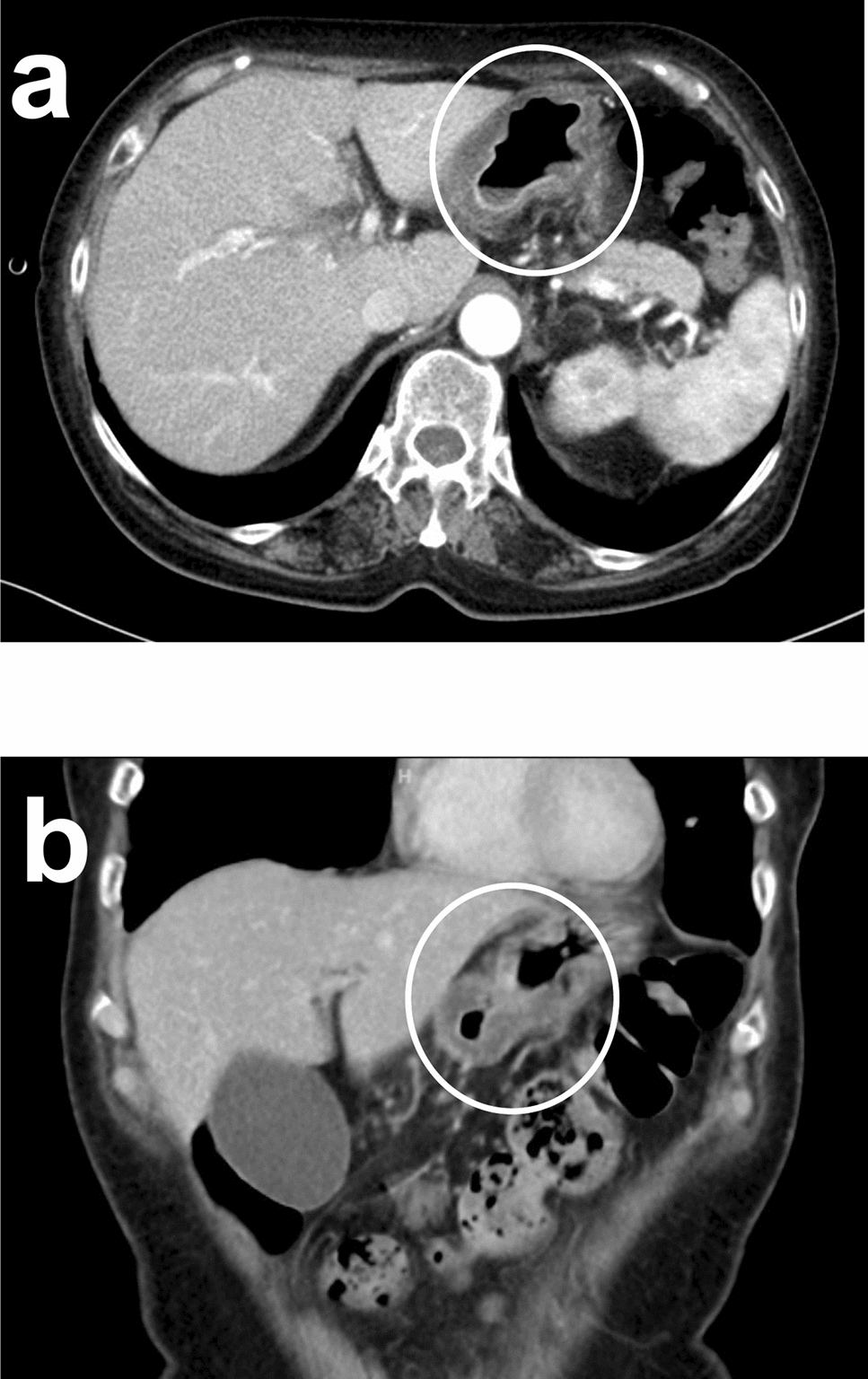
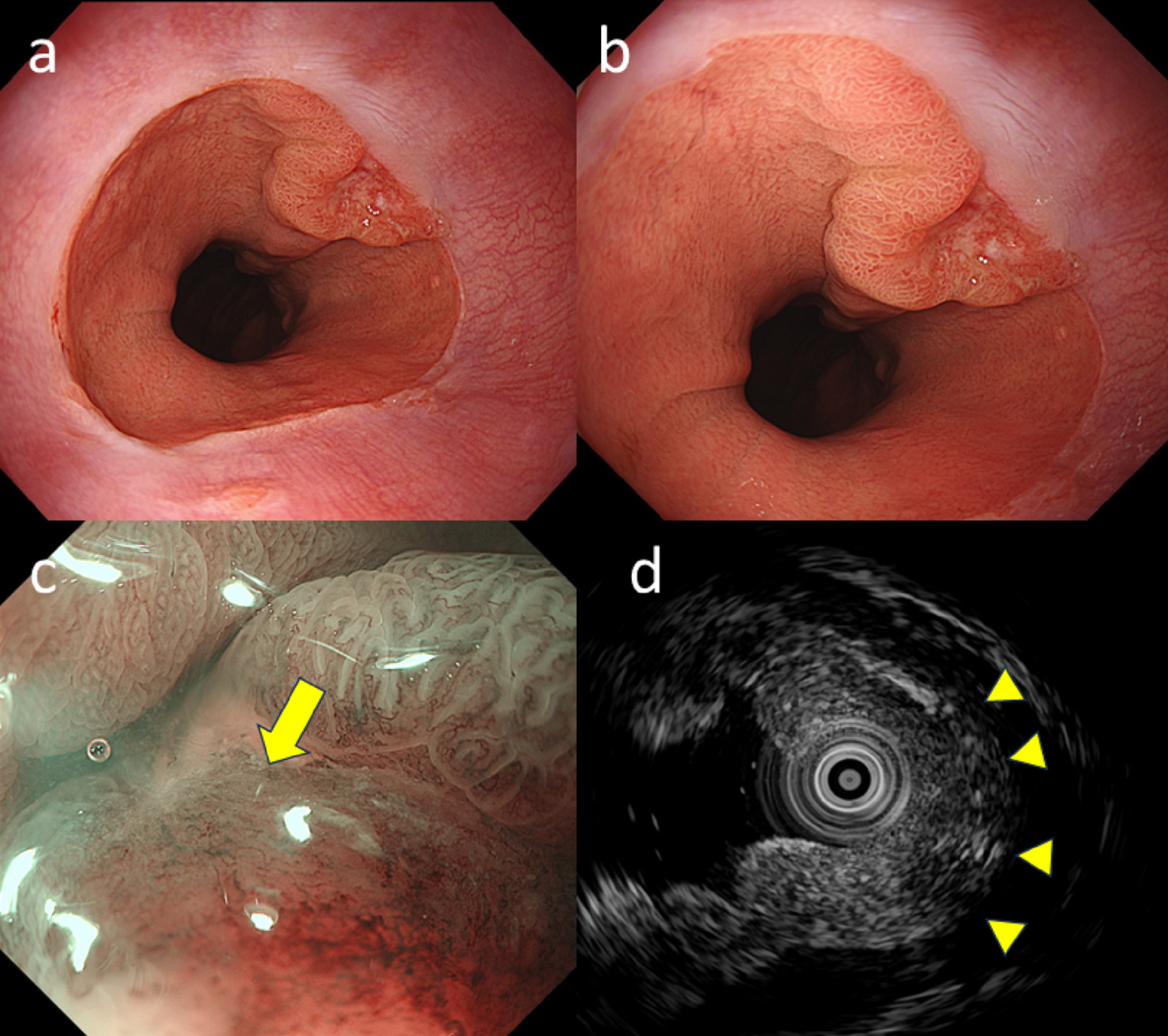
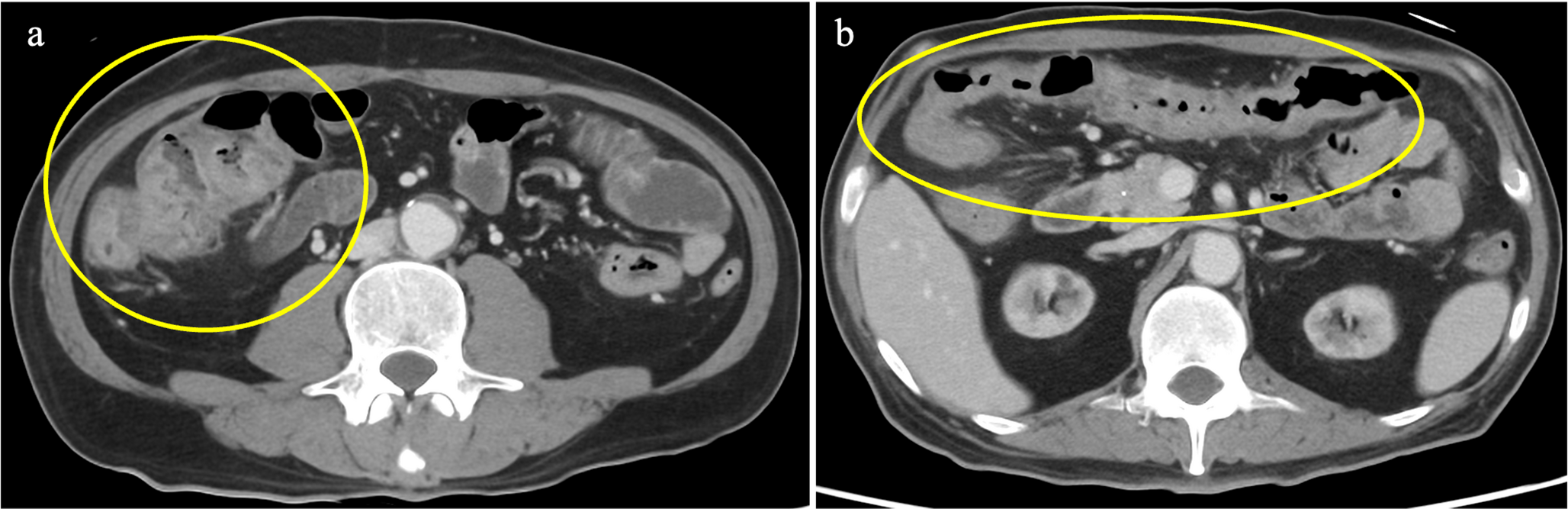
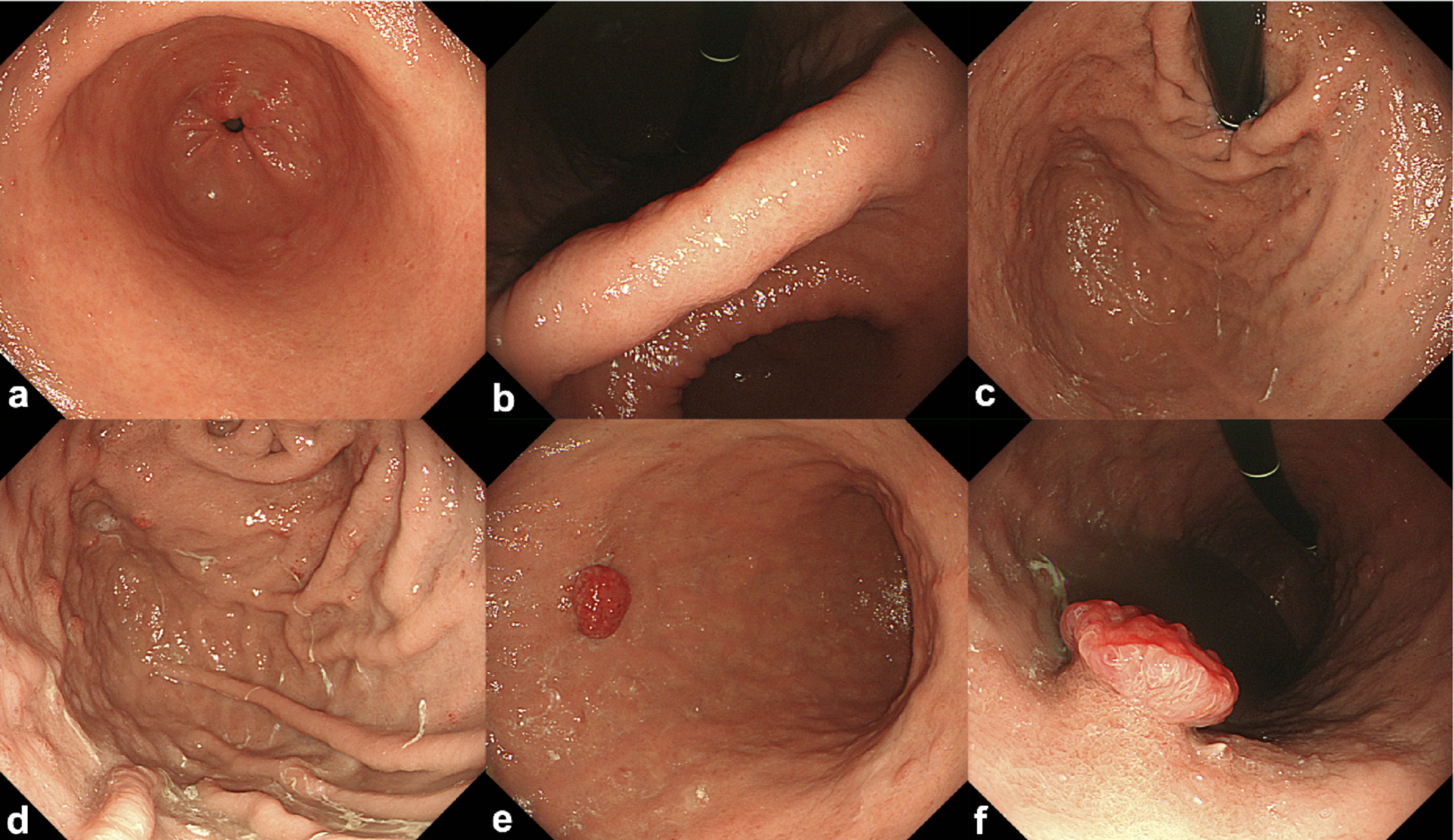
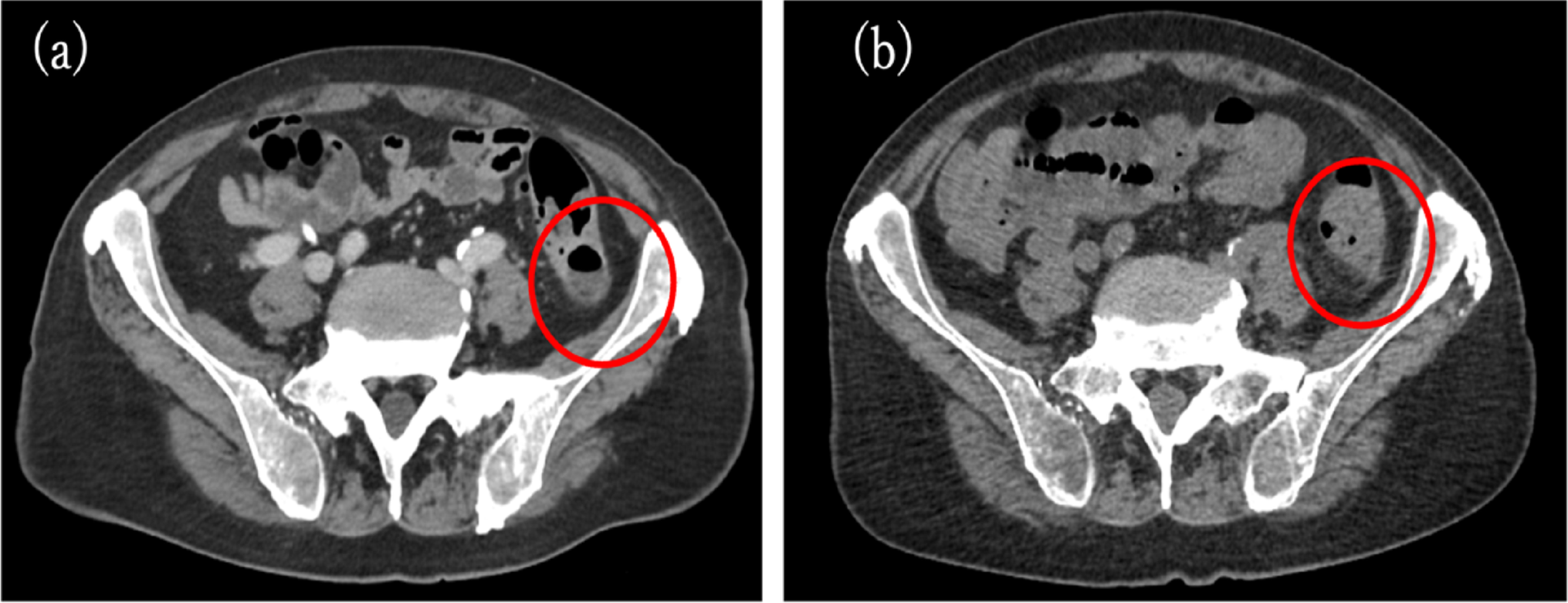
Gastrointestinal lymphomas most commonly present as ulcerative lesions with raised, ear-like margins, whereas other morphological patterns are less frequent. According to the endoscopic classification proposed by Kanno et al., the lesion observed in the present patient approximately 18 months before surgery was consistent with the ulcerative type, characterized by shallow ulceration with only mild mural thickening [26]. In contrast, the lesion at the time of surgery demonstrated circumferential and markedly thickened mural involvement, which did not clearly fit into any single category of this classification system, although it most closely resembled a diffuse infiltrative pattern. Such a morphology is considered extremely uncommon and may reflect an advanced stage of disease progression. Histological examination of biopsy specimens obtained both 18 months before surgery and at the preoperative endoscopy demonstrated inflammatory granulation tissue; however, retrospective pathological re-evaluation revealed scattered EBER-positive large cells in both biopsy specimens, indicating that EBV-driven lymphoproliferative changes were already present at an earlier stage, even when the lesion showed a morphology closer to the typical ulcerative pattern. In cHL, neoplastic Reed–Sternberg cells are typically sparse and embedded within a prominent inflammatory background, making them particularly difficult to distinguish from reactive inflammatory cells on routine hematoxylin–eosin staining. These findings suggest that reliance on routine histology alone may delay the diagnosis of EBV-associated cHL. Therefore, when gastrointestinal lymphoma is clinically suspected, close communication between clinicians and pathologists is essential. Clinicians should clearly convey their clinical suspicion and proactively discuss the indication for additional ancillary studies, including EBER in situ hybridization, to facilitate timely and accurate diagnosis.
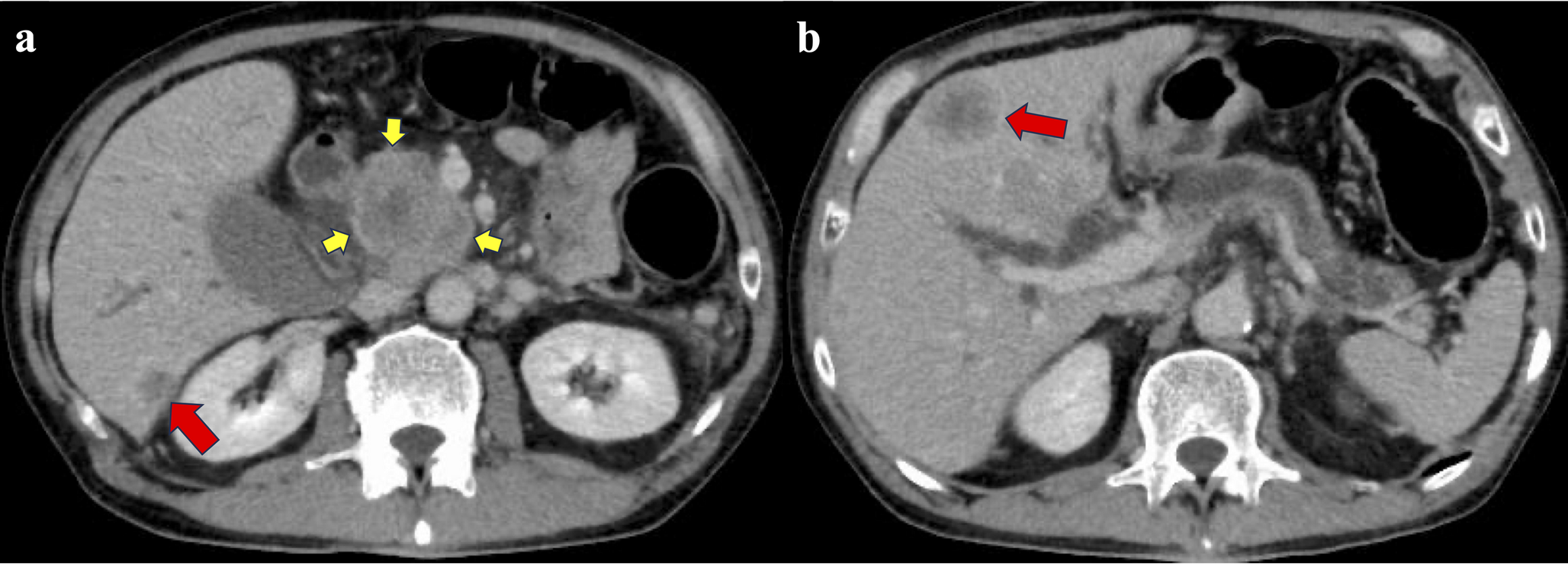
In conclusion, EBV-associated malignant lymphomas, including cHL, may develop in patients with UC receiving vedolizumab therapy; however, this report represents a single case, and a direct causal relationship between vedolizumab and EBV reactivation cannot be established. Despite this limitation, clinicians should maintain a high index of suspicion when lesions suggestive of neoplastic change, such as intestinal wall thickening with ulceration, are observed during vedolizumab treatment and should consider early histopathological evaluation with malignant lymphoma in mind to ensure timely and appropriate clinical management.

Comments (0)