
Remember me

While the focus of the analyses was on the qualitative outcomes, we calculated two quantitative measures to complement the findings. First, the number of comments assigned to each theme, which provides an indication of the relative emphasis placed on each topic in the discussion, noting that some participants can contribute more comments than others. Second, we calculated the percentage of participants who contributed comments under each theme.
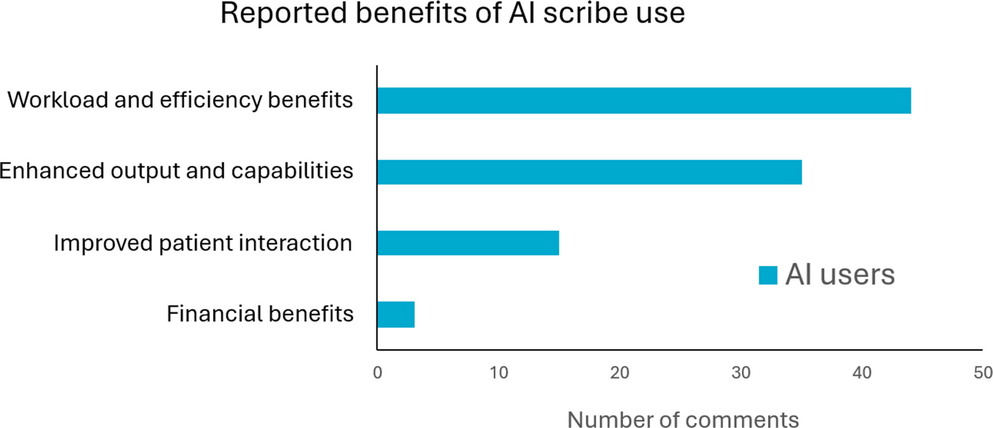
3.1 Benefits of scribe useAI users reported using scribes primarily for recording consultation notes, though some also use a scribe to craft referral letters. For some, scribes were implemented at the organisation level, but most began using them on their own initiative. Overall, AI users were positive about their experience, some referring to the tool as “life changing” and a “hallelujah moment”.
Fig. 1 shows the frequency with which each benefit was coded, providing an approximate indication of how much of the conversation centred on particular themes, and Table 2 shows the percentage of participants who contributed comments under each theme.
Fig. 1
Relative frequency of the reported benefits of scribes. Figure shows frequency of comment codeds under each benefit. Note data shown here is based on AI users, as benefits of scribes were not directly discussed with AI non-users
Table 2 Percent of AI Users and Non-users contributing comments in each themeTwo benefits were discussed most frequently and by almost all AI users. First, doctors felt scribes decreased workload and increased efficiency, with one participant noting a reduction in fatigue (see Table 3 for participant quotes illustrating each benefit). Some noted that scribes streamlined workflows by enabling them to edit notes during or immediately after consults, rather than waiting for dedicated note-writing time or outsourcing transcription. Secondly, scribes were reported to enhance work outcomes by enabling doctors to produce better notes or to compensate for limitations (typically, limited typing skills). Many reported being surprised and impressed by the comprehensiveness of the output and its ability to structure information and filter irrelevant “chit-chat”. Thirdly, doctors felt scribes improved their ability to focus on and engage with patients, with some patients even commenting on the improvement. Some felt describing symptoms out loud for the scribe also benefitted patients’ awareness. Finally, a small number of comments focused on financial benefits including saving money by not hiring transcriptionists or the capacity to see more patients.
Table 3 Benefits of scribe use with illustrative participant quotes3.2 Challenges to scribe use and facilitating factorsAs the focus group discussion of challenges had significant overlap with that of facilitators (e.g., challenges were often contextualised as a lack of a facilitating condition, such as lack of training), we combined these factors together. The initial data coding revealed a broad range of challenges and facilitators (see Supplemental Information for the full list). For conciseness, we combined these into six broad themes, discussed below. Fig. 2 shows the frequency of coded comments for each theme. Table 2 shows the percentage of participants contributing to each theme and Table 4 illustrative quotes.
Fig. 2
Relative frequency of the reported challenges of scribes summarised into key themes. Figure shows frequency of comments coded under each benefit
Table 4 Challenge themes with illustrative participant comments3.2.1 Insufficient knowledge of scribe technology and data managementBoth AI users and non-users reported gaps in their knowledge about AI scribes. Non-users felt they lacked information on which scribes are available, their accuracy, and how to use them effectively in clinical workflows, which contributed to reduced trust in the tools and a fear of being left behind as technology advanced. While users were naturally more familiar with how to use scribes, they lacked knowledge about how AI works “under the hood” (transparency) and whether scribes use the captured data for training, suggesting some important information is not acquired through experience alone. Many had formed hypotheses based on their own experiences or colleagues’ advice, which could lead to misconceptions about AI functionality and capability.
Data management emerged as a key knowledge gap for both users and non-users. This included where data is processed and stored (within Australia or overseas, which has implications for compliance with Australian privacy laws), storage duration, data ownership and access, and how the data is used. This was especially concerning for doctors in small medical practices who must make their own AI software choices, while those working in the public system or larger clinics can rely on internal support (e.g., IT department) to research and approve systems. Some doctors felt they would be unable to answer any questions from patients regarding data management or privacy, and this could harm the doctor-patient relationship.
FacilitatorsDoctors reported wanting more information from scribe vendors and trusted medical organisations (such as medical colleges or government agencies) on how AI systems work and how data is handled. Doctors felt that any guidance on AI should be backed by scientific evidence. Additionally, government-mandated requirements or a certification system would provide security to doctors that the tools had met some scrutiny, particularly those in private or small practices.
Peer learning, in the form of shadowing a colleague or observing a demonstration, was perceived to be highly valuable, more so than formal training. Trialling a system in a simulation, referred to as a “safe space” by one AI non-user, would enable doctors to build familiarity and develop strategies.
3.2.2 Presence of AI error and limited utilityAI users reported that scribes made errors reasonably frequently. These included misnaming medical terms (e.g., drug names), incorrect numerical values, formatting inconsistencies (e.g., switching between American and British English), omitting relevant data and hallucinations. Some errors had the potential for serious consequences; for example, one doctor reported that a scribe incorrectly recorded a patient’s left arm as needing an X-ray, rather than the right. On rare occasions a scribe added information (e.g., possible medications to prescribe), referred to by one doctor as “unsolicited advice”.
Non-users were concerned about AI errors, largely in response to media reports about AI or their experience with other AI tools. This contributed to a characterisation of scribes among some non-users as unpredictable, prone to hallucination (“going down rabbit holes”) and ultimately untrustworthy. Some non-users saw little utility in scribes, as they felt any efficiency gains would be offset by the additional work required to review and correct scribe outputs, while others felt they had become adept at managing their administrative work and did not need the extra tool.
FacilitatorsDiscussions around mitigating the risk of error tended to place the responsibility on doctors themselves. Both users and non-users felt it was imperative to thoroughly check and correct all AI outputs. To support this, some doctors suggested scribe vendors could provide statistics on the likelihood of different types of errors, which would enable doctors to calibrate expectations when using scribes and tailor how they reviewed output.
3.2.3 Medico-legal risks and responsibilitiesSome of the concerns raised by doctors were about the legal risks that may emerge from using scribes. Almost all doctors, including AI users and non-users, believed that they would be held legally responsible for any scribe-generate content that was entered into the medical record, which is consistent with their current legal obligations towards the accuracy of medical records in Australia [28, 29]. This created a significant barrier for some non-users, who did not wish to risk the legal consequences of failing to detect an AI-generated error.
Doctors raised various other medico-legal questions, suggesting that the broader legal framework for scribes remains unclear. These concerned liability in the event of a data breach, implications of editing AI output (e.g., whether this might be interpreted as changing the medical record), obligations to maintain up-to-date software and retrospective legal protections as technology evolves. There was some concern AI would cause a shift towards medico-legally defensive medicine, where protecting themselves against legal ramifications prevents doctors from acting in their patients’ best interest. Some felt governance and regulatory bodies have not been proactive in providing guidance, instead waiting for a legal precedent to define policy, while others thought technology is evolving too rapidly for policymakers to keep up.
FacilitatorsDoctors described a need for guidance on legal risks and responsibilities from insurers, professional bodies (e.g., medical colleges) and government agencies. Consistent messaging across these bodies would support broad awareness and acceptance, as not all doctors trust or access all sources. Information should be clear and accessible given doctors’ limited time for extensive research. Formal training on legal indemnity and data protection was also suggested.
3.2.4 Privacy concernsDoctors raised two privacy-related risks. First, non-users were concerned that information not appropriate for the medical record would nevertheless be transcribed. This included sensitive patient information, especially concerning family violence or mental health, but also information about the doctors themselves (e.g., “chit-chat” about their personal lives). The second risk, shared by both groups, related to data security. There was a fear, driven by recent high profile corporate data breaches, that private information could get into the “wrong hands”. Having the time and resources to gather information about the privacy risks was a continuing challenge for both AI users and non-users.
AI non-users believed privacy would be the biggest fear for patients, based on how patients reacted to technology change, referring in particular to the introduction of "My Health Record", an Australia-wide government online health data platform. They also felt that having a technology “listen in” on their conversation would inhibit patients from sharing information, and indeed some doctors (both users and non-users) reported having similar hesitancy with using scribes when they themselves received healthcare.
In contrast, AI users reported only a minority of patients were unwilling to consent to scribe use. They reported managing patient concerns by gaining consent on every use and pausing scribes when talking about sensitive issues. However, some users expressed concern that not all doctors were aware of the requirements around consent and confidentiality.
FacilitatorsDoctors felt they needed clear guidelines on what information should and should not be stored and processed with scribes. Greater transparency on how data is handled from scribe technology vendors and those administering the technology (e.g., health care practice owners and employers) would help doctors maintain privacy and better inform patients. Some doctors also suggested public-facing information campaigns from trusted government or medical bodies to help alleviate patient fears.
3.2.5 Overreliance and de-skillingAI non-users were worried that over time, doctors will come to over-rely on AI and accept its outputs uncritically, particularly when under time pressure. Doctors may also be biased towards accepting the AI output, especially under uncertainty or if they cannot accurately remember details from a consultation. AI users were less likely to express this concern, feeling they could actively and objectively evaluate AI output. Nevertheless, some statements made by AI users may imply overreliance; for example, interpreting something they did not recognise in the notes as their own mistake rather than AI hallucination, or paying less attention to details discussed in the consultation because they expected AI to pick it up (see quotes in Table 4).
A potential long-term risk of overreliance, expressed by both users and non-users, was the loss of skills required to critically evaluate AI output. Participants did not believe they would lose their own skills, even if not exercised as frequently (“it’s like riding a bike”). Rather, they were concerned future generations of doctors would fail to develop those skills.
FacilitatorsDoctors emphasised the importance of perceiving AI as a tool to assist (rather than replace) doctors in their work and maintaining active control over AI decisions. Several participants felt there was a need for concrete instructions on using scribes and reviewing outputs to prevent overreliance, and an identification of skills that may become more relevant (e.g., more descriptive communication in consults to support more effective transcription). One idea to prevent skill loss, already used in some institutions, was to limit students’ and junior doctors’ access to scribes, ensuring they develop necessary knowledge before using AI.
3.2.6 Loss of controlSome doctors, particularly non-users, feared that AI adoption could reshape professional roles in ways that reduced their agency and influence. These concerns were less about scribes and more about AI integration in healthcare generally, with scribes acting as a gateway to more advanced AI applications. Doctors worried that if AI becomes the standard of care, they may have less control to challenge AI or operate without it. Participants were concerned they may “lose their voice”, or their job may become less enjoyable with AI, especially if such tools are used to automate aspects of the trade that replace doctors’ skill. There were concerns about being pressured to adopt AI tools, whether by law, patients, management, or government, driven by expectations of efficiency and cost savings that may not be entirely realistic.
Additionally, some felt AI would change the doctor-patient relationship in negative ways. Patients may start questioning the role doctors play, particularly when they see doctors using such tools in their practice and believe they could use “Doctor ChatGPT” at home on their own. However, others were confident that patients’ preference for human interaction and the need for core clinical expertise (the “art of medicine”) would preserve the essential role of doctors.
FacilitatorsDoctors stressed the importance of conceptualising AI as an assistant and not a means to automate healthcare. Ideally, this philosophy would be held across the sector, including scribe vendors, medical bodies and the public, to help ensure the technology is purposefully designed to meet doctors’ needs and augment care, and to prevent top-down implementation of AI that undermines their autonomy. Doctors also wished to retain control over if and how they used AI, and to have a voice in decisions impacting their ways of working (e.g., increasing caseloads). Finally, doctors saw a need to actively develop new strategies and skills to employ AI most effectively and safely.
Comments (0)