
Remember me

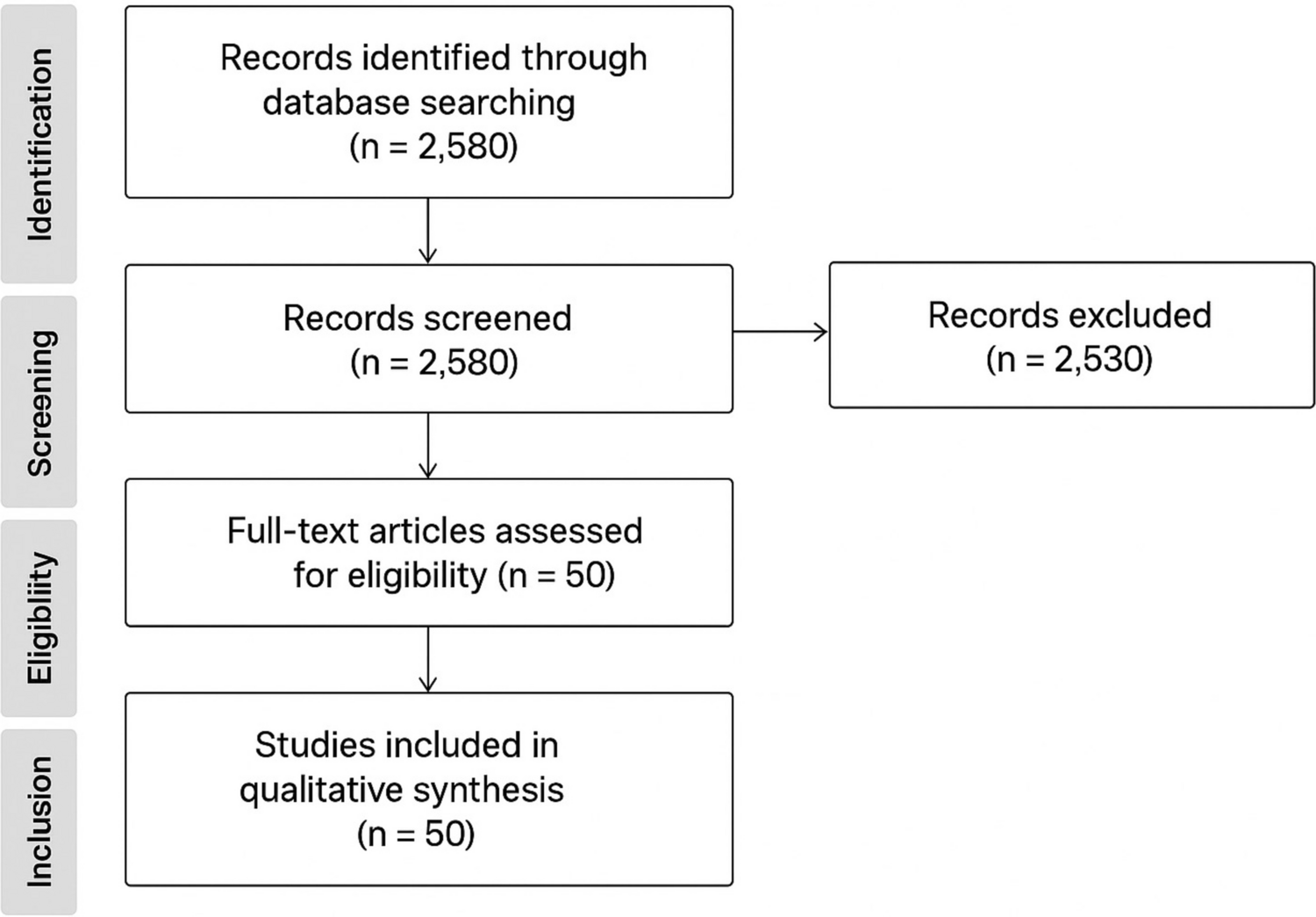
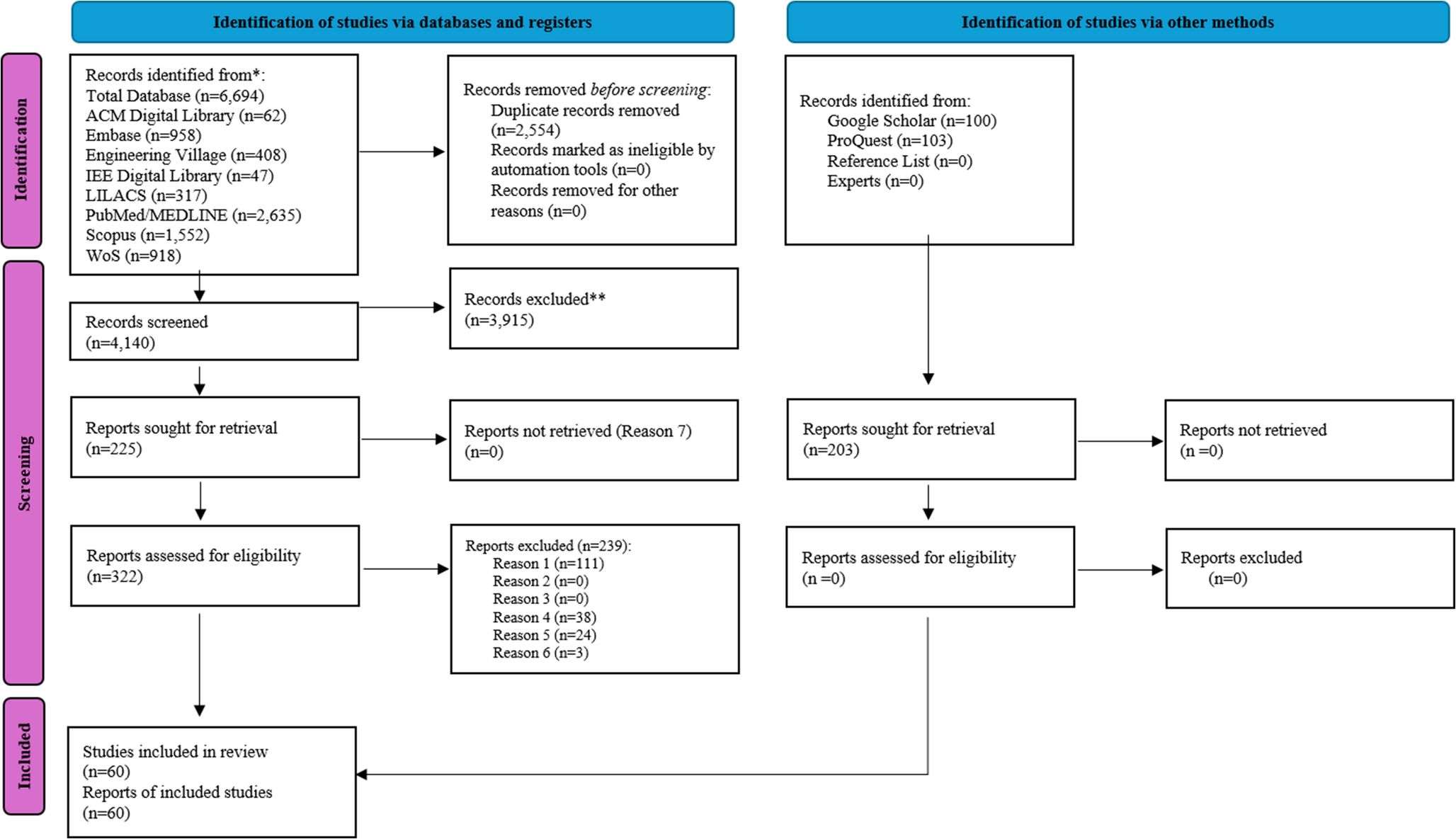
A total of 7, 100 articles were identified in the databases. After removing duplicate records, 4, 343 articles were screened by title and abstracts. A complete reading of 225 articles was performed, and 60 studies were included for descriptive synthesis (Fig. 1). Further information on the excluded articles and reasons for exclusion is available in Appendix 2.
Fig. 1
Flowchart of the literature search and inclusion criteria. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. Reason for exclusion: Reason 1. Studies that did not identify the telehealth system studied and/or only address health systems that do not cover a digital health strategy; Reason 2. Studies that address telehealth systems in the development phase and/or pilot phase in Brazil, not yet implemented in health systems, whether public or private; Reason 3. Studies that address only telehealth systems already implemented in countries other than Brazil; Reason 4. Studies that did not describe the characteristics of the system and/or its usability by health professionals; Reason 5. Studies that portray the use of telehealth only by users, without health professionals involved and/or established by channels/systems not specifically developed for telehealth purposes (generic video call systems, instant messaging applications, among others); Reason 6. Studies in the form of literature review articles (e.g., narrative review, systematic review, scoping review or overview), letter, book chapter, conference abstract, opinion article, article describing techniques, panel, brief communication, commentary, editorial, and clinical guidelines; Reason 7. Full text not found for full reading or correspondence authors not responding to the attempt to contact (three in a three-week period). From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: https://doi.org/10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/
3.2 Characteristics of sources of evidenceThe 60 articles were published in English (n = 52; 86.7%), Portuguese (n = 7; 11.7%), or Spanish (n = 1; 1.7%) between 2005 [23]and 2023 [23,24,25,26,27]. The studies were from 13 Brazilian states, mainly from the Southeast (n = 29; 48.3%) and South (n = 22; 36.7%). None of the studies examined the telehealth systems implemented in midwestern Brazilian states, the only region that was not represented by any study. Figure 2 illustrates the geographic distribution of telehealth systems in Brazil for a better understanding.
Fig. 2
The geographical distribution of Brazilian telehealth systems
Seven types of study designs were identified: descriptive studies (n = 30; 50.0%), analytical cross-sectional studies (n = 11; 18.3%), qualitative studies (n = 6; 10.0%), quasi-experimental studies (n = 4; 6.7%), case-control studies (n = 4; 6.7%), economic evaluations studies (n = 3; 5.0%), and cohort studies (n = 2; 3.3%), as listed in Table 1.
Table 1 Categorization of included articles based on study designThe articles were divided and classified by segments of telehealth systems (Table 2). Most articles identified telehealth tools from the teleconsultation segment (n = 39; 65.0%), followed by segments of telediagnosis (n = 16; 26.7%) and tele-education (n = 11; 18.3%). The remaining telehealth segments were less represented, appearing in fewer than ten studies: telemonitoring (n = 7; 11.7%), tele-electrocardiography (n = 6; 10.0%), teleassistance (n = 5; 8.3%), teledermatology (n = 3; 5.0%), teleradiology (n = 3; 5.0%), teleophthalmology (n = 3; 5.0%), telecardiology (n = 2; 3.3%), tele intensive care (n = 1; 1.7%), dental telehealth (n = 1; 1.7%), and telenursing (n = 1; 1.7%).
Table 2 Categorization of included articles according to the studied telehealth segmentsA complete detailed data referring to the individual studies characteristics are shown in Table 3 (Studies’ characteristics) and Table 4 (Systems’ specificities).
Table 3 Summary of the included articles’ characteristics (n = 60)Table 4 Summary of the descriptive characteristics of the telehealth systems (n = 60)3.3 Results of individual sources of evidence3.3.1 TeleconsultationThirty-nine studies were found. Twelve studies were conducted in Minas Gerais State [25, 28,29,30,31,32,33,34,35,36,37,38]. Of these, five [28, 29, 31, 33, 34] covered the Telehealth Network of Minas Gerais (TNMG) system. Three studies [30, 35, 38] focused on systems that promote the feasibility and projection of teleconsultations in the area of cardiology in the same state [30, 38] and the Telemedicine Infarct Network [35]. The remaining studies described the experiences, obstacles, and suggestions for teleconsultation systems implemented before [36, 37] and after the COVID-19 pandemic [25, 32].
Eleven teleconsultation systems were implemented in cities of Rio Grande do Sul State [23, 39,40,41,42,43,44,45,46,47,48,49]. Merlo et al. [45] assessed patient satisfaction using a questionnaire in the central region of the state, whereas, in three other studies [39, 42, 43], a public initiative was reported where attending doctors can discuss cases via teleconsultation or consult a doctor through an electronic platform or toll-free call. Three other studies reported on an ophthalmology teleconsultation system [40, 41, 46].
Only one study in Espirito Santo State [50] described a teleconsultation system that provides detailed communication among specialists and general practitioners. Seven studies were conducted in northeastern Brazil [24, 51,52,53,54,55,56], focusing on mobile applications [51], video-based teleconsultations [52], web-based systems [53], and the experience of the telehealth network [24, 54,55,56].
In Santa Catarina, three studies described the telehealth system [57,58,59], which includes a teleconsultation function, information systems, services, and modules that provide access to health and health education. One study covered Paraná and São Paulo states and aimed to facilitate physical examinations during teleconsultations [27]. Scudeller et al. [26] focused exclusively on São Paulo and reported implementing and expanding a tele-ICU program in Brazil. Lastly, only one study was conducted in the state of Amazonas and described the implementation of telehealth in the Forest Project by the Sustainable Amazon Foundation and the State University of Amazonas [60].
3.3.2 TelediagnosisThis adaptive method was covered in 16 studies. Santa Catarina had two studies that evaluated telehealth systems, ensuring usability, maintenance, efficiency, and reliable telediagnosis [57, 61]. Other studies described using telediagnosis and the DICOM system to generate and exchange diagnostic reports [62, 63]. During the COVID-19 pandemic, one study in a hospital in São Paulo offered telediagnosis services to patients in Recife [52], focusing on diagnosing COVID-19 symptoms and guiding patients toward appropriate treatment. Meanwhile, five studies conducted in Rio Grande do Sul explored different telediagnosis for mouth injuries and eye complaints or encompassed multiple fields of telehealth [40,41,42, 46, 64]. These studies emphasized the importance of diagnosis, especially for patients in remote areas.
In northeastern Brazil, researchers described an initiative network for cardiology diagnostics [54,55,56], where local pediatricians transmitted images and videos to remote specialists for treatment recommendations. In Minas Gerais, some articles reported telediagnosis in cardiology utilizing an asynchronous system where healthcare professionals uploaded images for assessment and received diagnostic reports from a centralized center [31, 33, 34].
3.3.3 Tele-educationMost articles (six out of eleven) were carried out in Pernambuco State. Four of them discussed the RedeNUTES system [54, 65,66,67], which includes tele-education for training in primary health units. The other two studies addressed the Regula + Brasil Project, evaluating teleconsultations in neurology [52], and the PC-Net, which researched the performance of the association between examinations together with online supervision in increasing the level of understanding of the pediatricians about echocardiograms [56].
São Paulo was featured in two studies. Prado et al. [68] presented a proposal for breastfeeding education, while Scudeller et al. [26] offered training on the care and treatment of COVID-19 patients. In Rio Grande do Sul, one study [42] also incorporated tele-education within the system for user training, and an article [25] covering Minas Gerais showcased a multifunctional system with tele-education capabilities for educating patients and healthcare teams. The only included study conducted in Amazonas described a project that supported isolated communities during the COVID-19 pandemic [60]. In Rio de Janeiro, Silva and Amorim [69] introduced an educational video conferencing system for pediatric radiologists in training. Lastly, one article [63] provided a comprehensive telehealth system providing various synchronous and asynchronous services in Santa Catarina.
3.3.4 TelemonitoringVarious healthcare contexts were examined concerning monitoring systems. For instance, Farias et al. [70] focused on a monitoring system for post-spinal surgery patients in São Paulo. The three studies conducted in Minas Gerais addressed a patient monitoring system within neonatal intensive care units [37], the usability of the system with healthcare professionals, identifying some deficiencies in SMS messaging [32], and the feasibility of implementing a public telecardiology system in small cities [38]. In contrast, three studies from Sachpazidis and collaborators [23, 47, 48] in Rio Grande do Sul presented a medical network system that collects patient images for remote monitoring and allows specialists to review patient exams remotely. Finally, two studies described a health monitoring center during the COVID-19 pandemic in São Paulo [71] and Minas Gerais [25].
3.3.5 Tele-electrocardiographySix studies covered tele-electrocardiography. Five were conducted in Minas Gerais, all authored by the same research group, and focused on a tele-electrocardiography system [28, 29, 72,73,74]. The studies discussed the challenge of professional adherence to the teleconsultation system [
Comments (0)