
Remember me
This prospective single-center cohort study was granted ethical approval by the institutional review board of the University Medical Center Rostock in line with the Declaration of Helsinki.
The study cohort comprised healthy adult subjects, including both genders, with a minimum age of 18 years and the capability of giving written informed consent. Exclusion criteria were defined as follows: presence of functional or structural heart diseases that directly or indirectly affect the heart, chronic lung or systemic disease (e.g., COPD, rheumatic diseases, etc.), pregnancy, or general contraindications for a magnetic resonance imaging (MRI) examination, such as non-MRI-capable implants.
The volunteers were selected based on equal gender distribution within the following predefined age groups: ≤ 34 years, 35–44 years, 45–54 years, and ≥ 55 years. Demographic data were documented prior to the first CMR scan. The heart rate was recorded during the examinations.
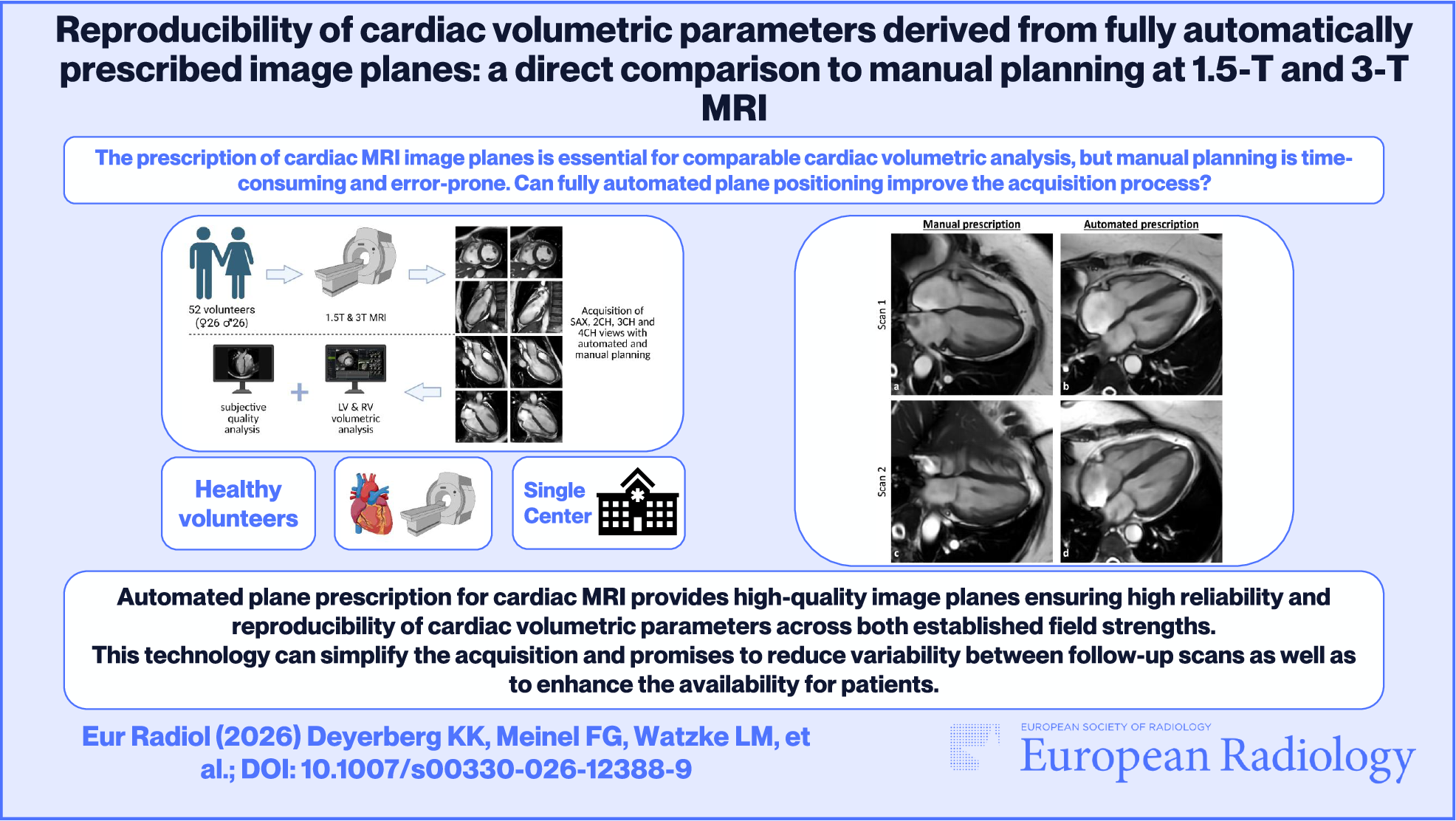
Study design and MRI protocolThe study design incorporates two identical CMR examinations. All participants underwent the first scan (hereinafter referred to as Scan 1) on a 1.5-T scanner (SIGNA™ Artist, GE HealthCare). For the second scan (hereinafter referred to as Scan 2) two sub-cohorts were established, as visualized in Fig. 1. The first subgroup (1.5 T sub-cohort) was established to assess the intra-field strength reproducibility and received the second CMR scan (Scan 2) on the same 1.5-T scanner used for Scan 1, with a time interval of two to five weeks. The scan interval was established with the objective of representing a clinically realistic interval. The second subgroup (3 T sub-cohort) aimed to assess the inter-field strength reproducibility, and Scan 2 was performed on a 3-T scanner (SIGNA™ Premier, GE HealthCare) directly after Scan 1 with a time interval of 1–2 h. The volunteers of the 3 T sub-cohort were not allowed to eat or drink between the two CMR scans to avoid any side effects on the cardiac function.
Fig. 1
Study design and cohort. Overview of the study design and both sub-groups. The 1.5 T sub-cohort received Scans 1 and 2 at 1.5-T field strength with an inter-scan interval ranging from two to five weeks. The 3 T sub-cohort received Scan 1 at 1.5-T and Scan 2 at 3-T field strength with an inter-scan interval ranging from 1 to 2 h. Two volunteers withdrew from participation before the second CMR scan. Five other volunteers were excluded due to incomplete coverage of the LV in the manual prescribed SAX image stacks, which resulted lack of a reference standard for volumetric results. The final cohort included 52 volunteers. Figure created with BioRender (https://app.biorender.com/)
The MRI protocol consisted of accelerated cine sequences (Sonic DLTM, GE HealthCare) with a three-heartbeat acquisition (3RR) and breath-holds [25], acquiring standard cardiac imaging planes including a left ventricular (LV) short-axis image stack (SAX) and single image planes in 2-chamber (2CH), 3-chamber (3CH), and 4-chamber view (4CH). Fully automated plane positioning was performed first, utilizing a prototype tool (AIRxHeart Prototype, GE HealthCare). Subsequently, the same cardiac image planes were acquired with manual prescription according to established imaging guidelines [16]. MR-protocol parameters for 1.5-T and 3-T field strength are summarized in Table 1.
Table 1 MRI protocol parameters at 1.5 T and 3 TAutomated AI-based plane prescriptionThe prototype tool for automated plane prescription (AIRxHeart Prototype, GE HealthCare) is based on a deep learning algorithm that can determine anatomical landmarks, such as the LV apex or the mitral valve. The algorithm first detects the heart position using the 3-plane localizer sequence. Anatomical landmarks, such as the mitral valve and LV apex, are then extracted from subsequent series using deep learning models that generate heatmaps indicating each landmark’s location. Although landmark detection is performed on individual image planes, this information is propagated and iteratively refined throughout the planning process. At each stage, the updated landmark positions are used to prescribe the geometry for the next acquisition. The user retains full control and can review or adjust the prescribed plane position and orientation at any time. The prototype version used in this study is capable of fully automated prescription of transverse image stacks, as well as pseudo-2CH, pseudo-4CH, SAX, 2CH, 3CH, and 4CH views.
Subjective image assessmentThe subjective quality of plane orientation was evaluated by two independent radiologists, each with a minimum of five years of experience in CMR, using an in-house browser-based tool in the same way described in a previous publication [26]. Examples of excellent and good quality image planes are visualized in Fig. 2. The results of the subjective quality assessment were analyzed for each plane separately and overall planes for both readers combined.
Fig. 2
Example of subjective quality rating criteria. Accelerated cine sequences in 3CH view of a healthy 56-year-old male acquired at 1.5 T. a Manually prescribed image plane with excellent quality of plane orientation and a subjective rating of 5/5. b Automatically prescribed image plane with a good subjective quality rating of 4/5. The aortic root and proximal ascending aorta are not perfectly visualized, but with no diagnostic impairments. This example demonstrates that, when evaluating the subjective plane orientation quality, both readers give a 5/5 rating only if the image plane has been prescribed perfectly. Therefore, the difference between a good (4/5) rating and a perfect (5/5) rating is not relevant for the diagnostic quality. 3CH, 3-chamber-view
Volumetric analysisVolumetric analysis of the LV and RV was performed fully automatically on SAX series using an established post-processing software (Cvi42, version 5.16, Circle Cardiovascular Imaging Inc.). The automatically generated contours were visually checked for plausibility, but no manual corrections were made. The papillary muscles of the LV were assigned to the blood pool, and the smooth segmentation preset was used. For quantitative assessment, the following parameters were determined for the LV and RV: end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), and ejection fraction (EF). Additionally, the diastolic mass of the LV was documented.
Statistical analysisThe statistical analysis was conducted with GraphPad Prism (version 10.3.1, GraphPad Software).
Verification of normal distribution using the Shapiro-Wilk test showed that body weight, height, and heart rate were normally distributed, while the majority of LV and RV volumetric parameters were not. Therefore, the non-parametric Wilcoxon Matched Pairs Signed Rank Test was used under a significance level of p < 0.05. Bland–Altman analysis was performed for the LV and RV volumetric parameters. The intraclass correlation coefficient (ICC) was used to assess the test-retest reproducibility of volumetric results derived from each planning approach. ICC values < 0.5 are considered poor, between 0.5 and 0.75 fair, between 0.75 and 0.9 good, and > 0.9 excellent [27, 28].
Comments (0)