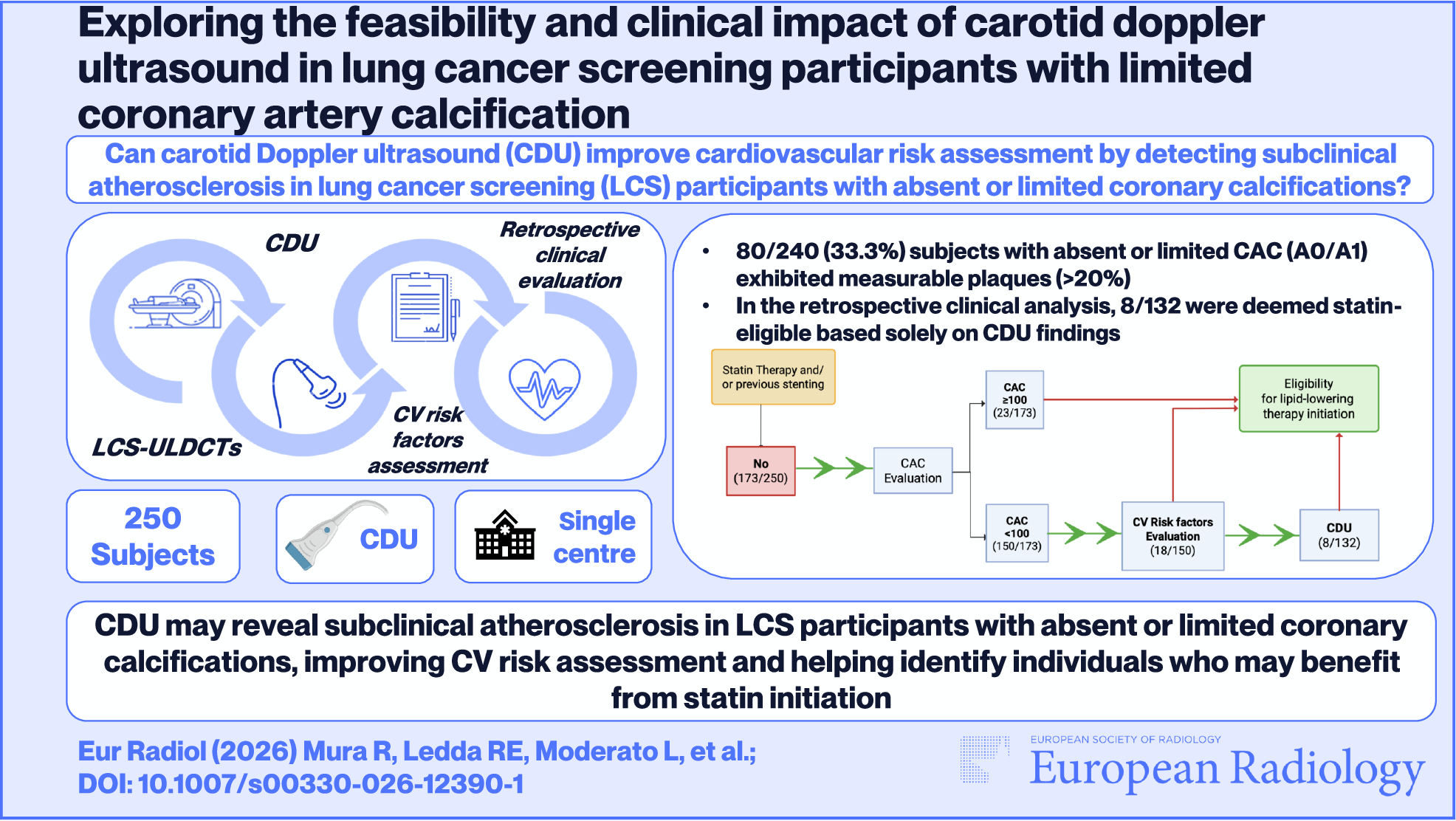
Based on the results of this prospective study conducted within an LCS setting, we observed that carotid plaques were frequently detected, with a prevalence of 49% (122/250) in the overall cohort. As expected, the burden of carotid plaques increased with higher CAC scores; however, we also confirmed the presence of subclinical atherosclerosis in participants with absent or limited CAC. Specifically, measurable carotid plaques were identified in one-third of subjects (80/240, 33.3%) with either no or limited CAC (18/240 A0, 62/240 A1), and 10 out of the 18 (55.6%) subjects with severe plaques were classified as A1. Unsurprisingly, approximately 75% of individuals categorised as A2/A3 exhibited measurable carotid plaques. Consistent with previous studies, these findings underscore the jeopardised distribution of subclinical atherosclerosis, especially among heavy smokers [14, 32, 33]. Moreover, of the eight subjects with echo-lucent plaques, 4 (50%) were classified as A0 and 2 (25%) as A1. Identifying these so-called “unstable plaques” can be clinically meaningful, as they are more frequently associated with an increased risk of acute ischaemic cerebrovascular events [34].
Our study findings highlight that CDU may provide additional value for identifying subclinical atherosclerosis even in apparently low-risk subjects such as those with no or limited CAC (categories A0/A1). Conversely, in individuals classified as A2/A3, further evaluation with CDU is unlikely to significantly impact treatment decisions or prognosis, as these are already considered at-risk [29, 30]. Indeed, CAC has been extensively investigated in the context of LCS, and the presence of moderate to severe CAC (categories A2/A3) has already been associated with both fatal and non-fatal CAD events [35,36,37]. Consistent with previous studies, the prevalence of CAC in our study’s cohort was 70.4% [38, 39]. Moreover, recent studies have further underscored the role of CAC in CV risk stratification, showing that its presence improves risk prediction even among individuals classified as low-to-borderline risk based on clinical scores alone [40]. However, the assumption that a calcium score of zero confers no CV risk might not be entirely accurate [41, 42]. In the LCS-eligible MESA cohort, 20.8% of subjects with an intermediate risk clinical score and no CAC experienced at least one CV event (including strokes and both fatal and non-fatal CAD events) after a mean of 11.1 years of follow-up [41, 43]. Notably, the 10-year CV event rate for this subgroup was nearly three times higher than that of the entire MESA cohort, highlighting the potentially significant impact of implementing primary prevention in LCS participants [44]. Moreover, previous studies assessing CV risk in LCS cohorts showed that a substantial proportion of individuals eligible for lipid-lowering therapy, or classified as intermediate risk based on clinical criteria, exhibited no detectable CAC [41, 44]. Thus, integrating various imaging modalities could enhance CV risk stratification, potentially prompting earlier initiation of lipid-lowering therapy.
According to Mehta et al, the heterogeneity in the long-term CV risk observed in individuals with absent CAC may be directly related to subclinical carotid atherosclerosis [11], and, as outlined by the 2021-ESC Guidelines, a more comprehensive atherosclerosis assessment by CDU can act as a risk modifier [15]. Based on these assumptions, we expanded our study to retrospectively investigate whether the systematic implementation of CDU within the LCS pathway could provide additional information to guide preventive treatment strategies beyond what can be derived from conventional CAC scoring. To the best of our knowledge, this is the first study to explore the complementary role of CDU in this setting.
Previous studies reported that up to 80% of LC-screnees who are eligible for lipid-lowering treatment were not receiving therapy, underscoring the potential of LCS programmes to serve as a broader “safety net”[43,44,45]. Similarly, nearly 70% of the study participants were not under treatment with lipid-lowering therapy. Based on CAC data, 23 subjects in A2/A3 groups (23/173, 13.3%) were eligible for starting lipid-lowering therapy, while, among A0/A1, a further 26 individuals (17.3%) were deemed eligible for lipid-lowering therapy based on CV risk factors (18/150, 12%) and CDU findings (8/132, 6%), respectively. These eight individuals, all classified as A1 (median 23 AU) and lacking significant conventional CV risk factors, were reclassified as eligible for lipid-lowering therapy solely due to CDU findings.
Although the proportion of individuals reclassified based on CDU was relatively modest (5%, i.e. 8/150), this finding may become clinically relevant when applied to larger populations. In the context of primary prevention, the number needed to treat (NNT) with statins to prevent one major CV event over 10 years ranges between 19 and 28 [46, 47]. This implies that even small increases in detection could yield significant clinical benefits. For instance, in the bioMILD trial, only 22% of more than 3000 individuals not receiving statins had CAC scores ≥ 100. If a similar 5% rate of CDU-based reclassification were applied to such a cohort, approximately 150 additional high-risk individuals could be identified. Based on an average NNT of 19–28, treating these patients could potentially prevent 5–8 major CV events, which can be regarded as clinically meaningful.
The global burden of CVD continues to rise, not only in terms of deaths and disability-adjusted life years, but also in costs, including healthcare and indirect costs, such as those related to lost economic productivity due to morbidity and premature mortality [48]. Participating in an LCS programme can represent a teachable moment to promote CVD prevention through lifestyle changes and initiation of primary prevention therapies [49]. This has been well-demonstrated, for example, by a sub-study from the ROBINSCA trial, which highlights how receiving a CT screening result increased participant prevention-seeking behaviour compared with traditional risk assessment [45, 49]. Building on this concept, adherence to our initiative was rather high, as only 10/335 (3%) subjects initially contacted declined the invitation.
However, while CDU remains a cost-effective, non-invasive, and radiation-free technique, its systematic implementation in all individuals classified as A0/A1 may raise concerns about feasibility. In our cohort, 150 CDU examinations were required to identify eight individuals with carotid plaques that would independently justify the initiation of a lipid-lowering therapy. This finding highlights both the potential value and the inherent limitations of CDU in the LCS scenario. Thus, although potentially reasonable from a clinical perspective, future strategies might benefit from a more targeted approach to optimise resource utilisation. In this light, optimising patient selection becomes a key challenge for future and sustainable applications of multidimensional approaches for improving CV risk stratification. The potential clinical impact of CDU seems most significant in participants with low or absent CAC in whom CT findings alone may underestimate subclinical atherosclerosis. Within this subgroup, adding specific imaging characteristics—such as emphysematous changes or aortic calcification—might help refine selection for additional US evaluation. Although our study was not designed to identify such predictors (as we prospectively performed CDU without preliminary evaluation of other imaging descriptors), exploring these correlates could be a valuable direction for future research, supporting a tailored approach to CV risk assessment in LCS populations.
This study has some limitations. First, it is a single-centre study with a relatively small population. Second, conventional CV risk factors were self-reported through a health questionnaire. In particular, we observed some inconsistencies as three subjects reported a history of coronary stenting but no lipid-lowering therapy. Furthermore, due to the relatively short follow-up, information on subsequent CV events was not collected, and further cost-effectiveness analyses were not performed, as they were beyond the scope of the present study.
In conclusion, our study results reveal a sizeable proportion of subjects with carotid plaques in participants of an LCS programme, confirming the presence of subclinical atherosclerosis even in individuals with absent or limited CAC.

Comments (0)