
Remember me
This study used data from the UK Biobank, a large-scale prospective cohort study that recruited over 500,000 participants aged 40–69 years across England, Scotland, and Wales in the UK between 2006 and 2010. At baseline, participants completed touchscreen questionnaires, which collected their sociodemographic characteristics, lifestyle behaviors, and medical information. Health-related outcomes were followed through linked data from national databases, including primary care systems, hospital admission records, and death registers. The UK Biobank has received approval from the North-west Multi-Centre Research Ethics Committee. All participants provided informed consent at the recruitment visit, and records of those who withdrew were removed. This cohort study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
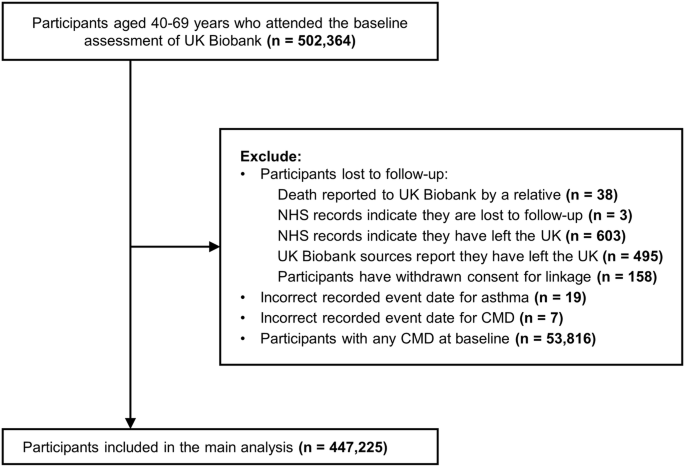
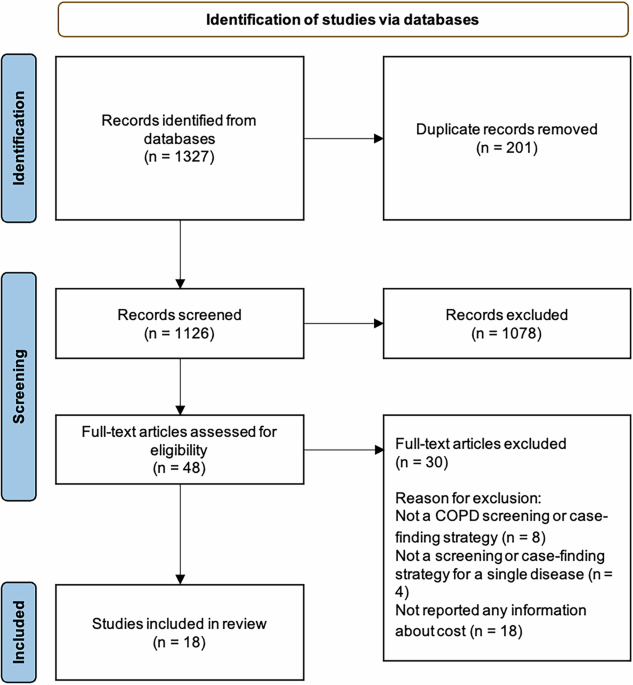
We included all participants who completed the baseline assessment (n = 502,364), excluding those lost to follow-up (n = 1,297), those with incorrected event date for asthma (n = 19) or CMD (n = 7), and those with any CMDs at baseline (n = 53,816). In total, 447,225 participants were included in the analyses of the associations of asthma with incidence and transitions to CMM. Figure 1 displays the detailed study design.
Fig. 1: Study flowchart.
CMD, cardiometabolic disease; NHS, national health service.
Ascertainment of asthmaWe ascertained asthma (ICD-10 code J45) using first-occurrence data derived from primary care records, inpatient hospital records, death register data, and self-reported medical conditions (Table S1). Based on the age at asthma diagnosis, we further classified asthma into childhood-onset asthma (COA, <18 years) and adulthood-onset asthma (AOA, ≥18 years). Due to limited records of early-life disease registries in the UK Biobank, asthma history was primarily determined based on self-reported information in the current study. Previous studies support the validity and reliability of self-reported asthma in the UK Biobank17.
Ascertainment of cardiometabolic multimorbidity and deathIn line with previous studies18,19, CMM was defined as the co-occurring of two or more of the following CMDs: T2DM, CHD, and stroke. Information about CMD diagnosis was obtained from first occurrence fields and coded according to the ICD-10: T2DM (E11, E14), CHD (I20-I25), and stroke (I60-I64, I69) (Table S1). The incidence of CMM was defined as the onset of CMM for participants who were free of any CMD at baseline. We also defined three CMM incidence-derived outcomes: CMD counts (0, 1, 2, and 3 CMDs), CMM patterns (a. none; b. only T2DM; c. only CHD; d. only stroke; e. T2DM and CHD; f. CHD and stroke; g. T2DM and stroke; h. T2DM, CHD, and stroke), and transitional phases of CMM progression.
Death information was obtained from death certificates held within the National Health Service Information Centre (England and Wales) and the National Health Service Central Register (Scotland).
CovariatesCovariates assessed in this study included sociodemographic (age at baseline, ethnicity, recruitment center, education level, and Townsend deprivation index), lifestyle (smoking status, drinking status, physical activity, intake of fruits and vegetables, and sleep duration), and early-life factors (breastfed, part of multiple births, maternal smoking around birth, and family history of CMD). Responses of “don’t know” or “prefer not to answer” for these covariates were considered missing and classified into the “unknown” group. Inhaled corticosteroids (ICS) are the first-line treatment for asthma, but they are associated with adverse cardiometabolic outcomes. Therefore, we extracted self-reported information on the use of ICS at baseline. Further details of the measurement of covariates are provided in Table S1.
Statistical analysisThe baseline characteristics of the participants were summarized according to asthma and CMM. Continuous variables were summarized as mean ± standard deviation (SD), and categorical variables were summarized as frequency (percentage). Differences between groups were compared using the Student’s t-test or Chi-square test, as appropriate.
After we assessed the proportional hazards assumption, we used Cox proportional hazards models to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations of asthma with CMD and CMM. Years from baseline to the onset of CMD, CMM, death, or the end of the follow-up (31st December 2022), whichever occurred first, were considered the time scale. Schoenfeld residuals indicated no violations of the proportionality assumption. We further used multi-state models to estimate the association between asthma and transitional phases of CMM progression. In line with the previous study20, five transition stages were constructed, including a. baseline to first CMD (FCMD); b. FCMD to CMM; c. baseline to death; d. FCMD to death; and e. CMM to death (transition pattern A, Fig. 2A). For participants entering different stages on the same date, we calculated the entering date of the theoretically prior state as the date of the latter state minus 0.5 day20. We also divided the FCMD into three individual diseases, constructing eleven transitions (transition pattern B, Fig. 3A). In this transition pattern, we excluded 1489 participants diagnosed with at least two CMDs on the same date, as we could not determine the temporal sequence of the CMDs. All models were adjusted for age, sex, ethnicity, region, education level, Townsend deprivation index, smoking status, drinking status, physical activity, intake of fruits and vegetables, breastfed, part of multiple births, maternal smoking around birth, and family history of CMD. We also did separate analyses for the male and female cohorts.
Fig. 2: Association between asthma and transitional phases of CMM progression (pattern A).
A. Numbers (percentages) of participants in transition pattern A; B. Forest plot for the association between asthma and five transitional phases. FCMD, first cardiometabolic disease; CMM, cardiometabolic multimorbidity; HR, hazard ratio; CI, confidence interval.
Fig. 3: Association between asthma and transitional phases of CMM progression (pattern B).
A. Numbers (percentages) of participants in transition pattern A; B. Forest plot for the association between asthma and eleven transitional phases. T2DM, type 2 diabetes mellitus; CHD, coronary heart disease; CMM, cardiometabolic multimorbidity; HR, hazard ratio; CI, confidence interval.
We conducted subgroup analyses to assess the association between asthma and CMM stratified by age (<60 and ≥60), recruitment center (England, Scotland, and Wales), ethnicity (White and non-White), TDI (quintile 1 to quintile 5), and education level (college or university degree and other qualifications). The interaction effects were evaluated by performing analyses of variance comparing regression models with and without interaction terms21.
We also conducted several sensitivity analyses to assess the robustness of the longitudinal analyses. First, we excluded participants who developed CMM within 2 or 4 years to reduce potential reverse causation. Second, we conducted competing risk models, wherein death before CMM was set as the competing event. Third, to test the influence of missing values, we excluded participants with missing covariates. Fourth, we assumed that missing data were missing at random and imputed missing covariates using multiple imputation, generating five complete datasets, with results combined according to Rubin’s rules. Table S2 presents the frequency of participants by the number of missing covariates. Fifth, we only included participants who did not use ICS. Sixth, we redefined T2DM using ICD-10 code E11 as the criterion instead of E11 and E14. Finally, we restricted the events of interest to those identified solely from hospital diagnosis records.
All analyses were performed using R software (version 4.4.0). A two-sided P < 0.05 was considered statistically significant.
Ethics approval and informed consentAll participants in the UK Biobank provided informed consent. The UK Biobank has ethical approval from the North-West Multicenter Research Ethics Committee. All methods were performed in accordance with the relevant guidelines and regulations.
Comments (0)