
Remember me
The 2019 GINA Strategy8 heralded a major shift in asthma management amongst concerns about the overuse of short-acting Beta -2 agonists increasing the risk of severe asthma exacerbations9.
A large-scale randomised controlled trial10 demonstrated the superiority of as-needed inhaled anti-inflammatory reliever(AIR)therapy using low-dose budesonide/formoterol in reducing asthma exacerbations compared to short-acting beta-2 agonists (SABA) alone. Similarly, a large real -world study11 showed that AIR therapy significantly reduced severe exacerbations compared to traditional ICS plus SABA reliever therapy. In patients with moderate asthma, regular maintenance and as-needed reliever therapy (MART) with budesonide/formoterol further reduced exacerbations compared to traditional therapy with maintenance ICS or ICS/long-acting beta-2 agonist (LABA) plus on-demand SABA12. As a result, GINA recommends a major shift in asthma management from maintenance ICS with SABA reliever therapy to ICS/formoterol as single reliever therapy (AIR) in mild asthma and as maintenance and reliever therapy(MART) in more symptomatic patients.
The BTS/NICE/SIGN Guideline group has also carried out an economic analysis of the interventions and has found that AIR and MART are “dominant” i.e. more effective and cost less, han corresponding SABA therapy alone or maintenance ICS or ICS/LABA plus SABA therapy.
This analysis gives major support by BTS/NICE/SIGN for the GINA recommendations and shows that AIR and MART therapy are not only effective,but also cost-effective. (albeit based on United Kingdom costs).
GINA and BTS/NICE/SIGN both recommend similar preferred management pathways and are shown in Fig. 2. Initial treatment should be commenced with AIR therapy if symptoms are relatively infrequent and with low or medium -dose MART if symptoms are more persistent, there is night waking or post-exacerbation, although the evidence for the efficacy of this treatment approach is relatively lacking.
Fig. 2: Preferred pharmacological management.
Preferred pharmacological management of asthma in adults and adolescents (12 and over GINA)1 and adults and young people (12 and over BTS/NICE/SIGN)2.
They both emphasise the need for checking factors such as adherence, inhaler technique, trigger factors and diagnosis before escalating therapy and also considering of stepping -down therapy when a patient is “stable’ (after 3 months-GINA).
However, there are some differences:
GINA recommends an alternative treatment pathway (“Track 2”) to AIR and MART therapies, based on the traditional maintenance ICS and SABA relief therapy. However there is no Track 2 in the NICE/BTS/SIGN guidance for people with asthma age 12 and over.
GINA does not recommend adding LTRA or LAMA to moderate-dose MART (≤ 800 mcg per day of Beclometasone or equivalent7 via DPI or standard-particle MDI before specialist referral. However, BTS/NICE/BTS suggest trying these options before referral unless FeNO is raised. (suggesting poor adherence with ICS or a need for additional anti-eosinophilic inflammatory drugs)
Overall the NICE/BTS/SIGN Guideline for management of asthma in people age 12 and over gives support for the GINA approach of single ICS/formoterol AIR and MART therapy as the core asthma treatment for chronic asthma management. However, this may not be applicable in lower economy countries where availability and cost of combination ICS/LABA inhalers may be problematic. In these case GINA’s alternative treatment pathway centred around maintenance ICS and relief SABA use may be more relevant.
The recommended pharmacological management by GINA and BTS/NICE/SIGN is shown in Fig. 3. The GINA approach is always to use inhaled corticosteroids in addition to bronchodilator when the child is symptomatic, progressing to regular ICS and SABA as needed and MART with increased asthma severity. The BTS/NICE/SIGN approach advocates regular ICS and SABA as-needed for mild asthma progressing to MART therapy. Both strategies recommend low-dose MART therapy as an initial treatment for highly symptomatic children.
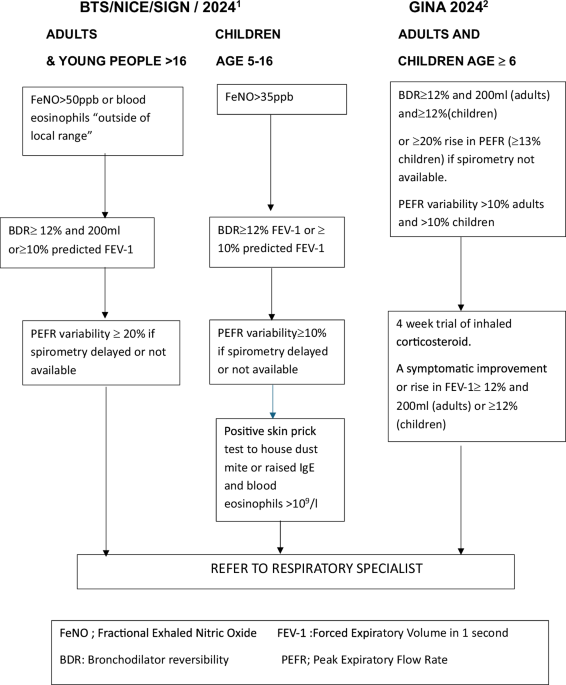
Fig. 3: Preferred pharmacological management.
Preferred pharmacological management of asthma in children age 6–11(GINA)2 and children age5–11(NICE/BTS/SIGN)1.
There are limited studies on the use of MART in this age group13 although an economic analysis was carried out by NICE which shows that MART therapy is cost-effective. At the time of writing (December 2024) MART is not licensed for younger children in the United Kingdom. In view of the concerns about the effects of SABA therapy without concomitant ICS in adults the GINA approach of always giving a form of ICS (either separately or in combination with bronchodilator) with relief medication does seem sensible although evidence to support this is limited14
Comments (0)